Āyurveda
Prevention and management of cardiovascular disease in post-menopausal women through Āyurveda
Abstract
The post-menopausal period of a woman’s life is more vulnerable due to aging as well as the inevitable scars of menopause. This period is associated with a significant increase in the incidence of age-related medical conditions like cardiovascular diseases and osteoporosis. Cardiovascular disease (CVD) in post-menopausal women is under-diagnosed and under-treated as the clinical features differ in men and women. Diagnosis at a later stage makes the condition difficult to manage and, as a result, there is an increase in the number of deaths in post-menopausal women due to heart-related conditions. Reviewing Āyurvedic literature to understand the disease reveals kaphaja hṛdroga and medāvṛtta vaata as conditions near to post-menopausal cardiac disorders. Use of phytoestrogens in managing various post-menopausal complications encourages extensive use of herbs like Śatāvari in preventing and managing life-threatening diseases like cardiovascular disease and osteoporosis.
Women, throughout their reproductive, menopausal and post-menopausal stages, are constantly subjected to various physiological and psychological changes. Old age becomes a more vulnerable period for women because along with aging, they have to suffer from the inevitable traumas of menopause. Women’s lives are very closely linked to the female sex hormones, i.e. oestrogen and progesterone. Menopause, the permanent loss of menstruation after amenorrhea, lasting more than one year due to the loss of oestrogen production by the ovaries, is a major aging process in women and most women encounter this hormonal change between 40 and 55 years of age (1). Therefore, many women spend almost one third of their lives in the post-menopausal stage. As women age, they are more likely to experience disease and disability (2). Because of significant alterations in body functions, women have many diseases and disabilities requiring intervention and treatment after menopause (3). Diseases in older women that are hormone-dependent include osteoporosis, Alzheimer’s disease, urinaryincontinence, and coronary atherosclerosis.Men vs women in cardiovascular health
Women during their reproductive years are at lower risk from coronary heart disease than men but this difference tends to disappear after menopause. Studies show that heart disease kills six times as many more women than breast cancer (4,5). Also, the number of women affected by heart disease is growing with changing lifestyles. Heart disease is the number one killer of women, and often acts differently than the way it affects men.
The incidence of CVD in Indian women has been noted to have significantly risen. Projected deaths from CVD by 2020 are estimated to be 42% of the total deaths. One in nine women (aged 45-64) have some form of cardiovascular disease. After age 65, the odds climb to one in three (6).
Why the gender gap?
Women tend also to take their symptoms less seriously. Health professionals often do not recognise the warning signs until they are too late. Women receive fewer interventions to prevent and treat heart disease, including fewer cholesterol screenings, fewer lipid-lowering therapies, and fewer referrals to cardiac rehabilitation. Only 33% of women diagnosed with CVD receive angioplasty whereas 36% undergo open heart surgeries. 38% of women die after an attack as compared to 25% in men. Also a recurrent attack is seen in 35% of women with only 18% in the case of men (7).
Protective effect of oestrogen during reproductive phase
Epidemiological studies on gender differences show the protective effects of oestrogen by increasing high density lipoprotein (HDL) and decreasing low density lipoprotein (LDL) and total cholesterol. It also inhibits platelet and macrophage aggregation at the vascular intima. Oestrogen stimulates release of nitric oxide and prostacycline from vascular endothelium to dilate blood vessels and prevent atherosclerosis by antioxidant property. Oestrogen decreases renin, ACE, endothelin-1, and vascular expression of angiotensin receptor type 1, with the net effect of promoting vasodilation.
After menopause, the production of oestrogen by the ovaries gradually diminishes over several years. Along with this reduction, there is an increase in LDL (‘bad’ cholesterol) and a small decrease in HDL (‘good’ cholesterol). These changes in lipid levels are believed to be one of the reasons for the increased risks of developing coronary artery disease (CAD) after menopause. Changes in cardiac function after menopause due to atherosclerosis are decreased myocardial contractility, decreased stroke volume, decreased peak flow velocity, and decreased left ventricular function.
Women who have had their ovaries surgically removed or experience an early menopause also have an accelerated risk of CAD.
Risk factors for cardiovascular disease (CVD)
The risk factors for cardiovascular disease are divided as modifiable and non-modifiable. Sex, age, ethnicity and genetic factors are considered to be the non-modifiable risks whereas obesity, hypertension, diabetes, stress, smoking, sedentary lifestyle, and dyslipidaemia are modifiable factors. Being female itself and the post-menopausal period are independent risk factors for CVD in women.
Diabetes
Women with diabetes have seven times more cardiovascular events than other women and about half of them die of CVD. Women with diabetes and CVD, especially Hispanic and African-American women, die at a much higher rate than men or non-diabetic women. Young women with diabetes lose any pre-menopausal protection.
Hypertension
This puts women at a much greater risk from CVD, especially if it develops before menopause. At least half of women may have hypertension before menopause. Elevated blood pressure is two to three times more common in women who take oral contraceptives, especially older women who are overweight.
Smoking
Even a few cigarettes a day correlate with a greater risk of CVD or fatal myocardial infarction1 (MI). About one-quarter of all women smoke; prevalence is greatest among post-menopausal women. Younger women who smoke probably cancel out any pre-menopausal protection. Women who take oral contraceptives and smoke are more likely to have an MI or stroke than those who take the pill but don’t smoke.
Dyslipidemia
This doubles a woman’s risk of CVD compared to women with normal lipid profiles. Low levels of HDL have been shown to be a much stronger predictor of CVD mortality in women than men.
Obesity
Central obesity poses a greater risk than increased body mass index (BMI). A healthy waist circumference in women is less than 35 inches; in men, less than 40 inches. The desired BMI (men and women): 18.5 to 24.9 kg/m2 (8).
Sedentary lifestyle
This can contribute to obesity, dyslipidemia, hypertension, and hyperglycemia. Exercise can reduce cardiovascular risk by increasing HDL and decreasing blood pressure, blood glucose, and LDL. Exercise can cut a woman’s CVD risk by half and may significantly decrease the risk of a second MI in a post-menopausal woman
Stress
This puts a woman at greater risk for CVD and poorer outcomes. Depression also may increase risk or deter her from seeking medical help. The screening of women for CAD should be done earlier in cases of depression for early referral for treatment as needed.
Symptoms of CVD in women
During heart attacks, women experience nausea, vomiting, indigestion, shortness of breath or extreme fatigue, but surprisingly frequently no chest pain. Unfortunately, these symptoms are easy to attribute to something other than the heart. Women are also more likely than men to have ‘silent heart attacks’ — an attack without any acute symptoms, that are diagnosed only later when subsequent cardiac symptoms are re-evaluated and tests are performed.
Men |
Women |
| Classic substernal pain | Shortness of breath |
| Heaviness in chest | Fatigue |
| Crushing and squeezing feeling in chest | Changes in sleeping patterns |
| Commonly occurs with physical exertion or emotion | Heaviness, squeezing, or pain in left chest, abdomen, mid-back, or shoulder |
| In cases of MI, pain can occur while resting |
Arm pain |
| Sharp or fleeting palpitations or pain |
Hormone therapy and cardio-protection
Hormone therapy is not a viable intervention for the primary prevention of coronary heart disease (CHD). It does not reduce or slow the progression of established CHD. It is also recommended as a conclusion of trials done by Women Health Initiative under HERS I and HERS II (the Heart and Estrogen Progestin Replacement study) that post-menopausal women with existing atherosclerosis should not be given hormone therapy. (9,10).
Research studies conducted on the management of CVD in post-menopausal women with alternatives like SERMs (Selective Estrogen Receptor Modulators) such as Raloxifen and Tamoxifen showed increases incidences of venous thromboembolism, DVT and pulmonary embolism. (11,12)
Understanding cardiovascular disease in post-menopausal women — an Āyurvedic perspective
As the causative factors, nature of occurrence and symptoms of cardiovascular disease in post-menopausal women are different from men, it is necessary to understand the etiological factors and pathogenesis on the basis of Āyurveda.
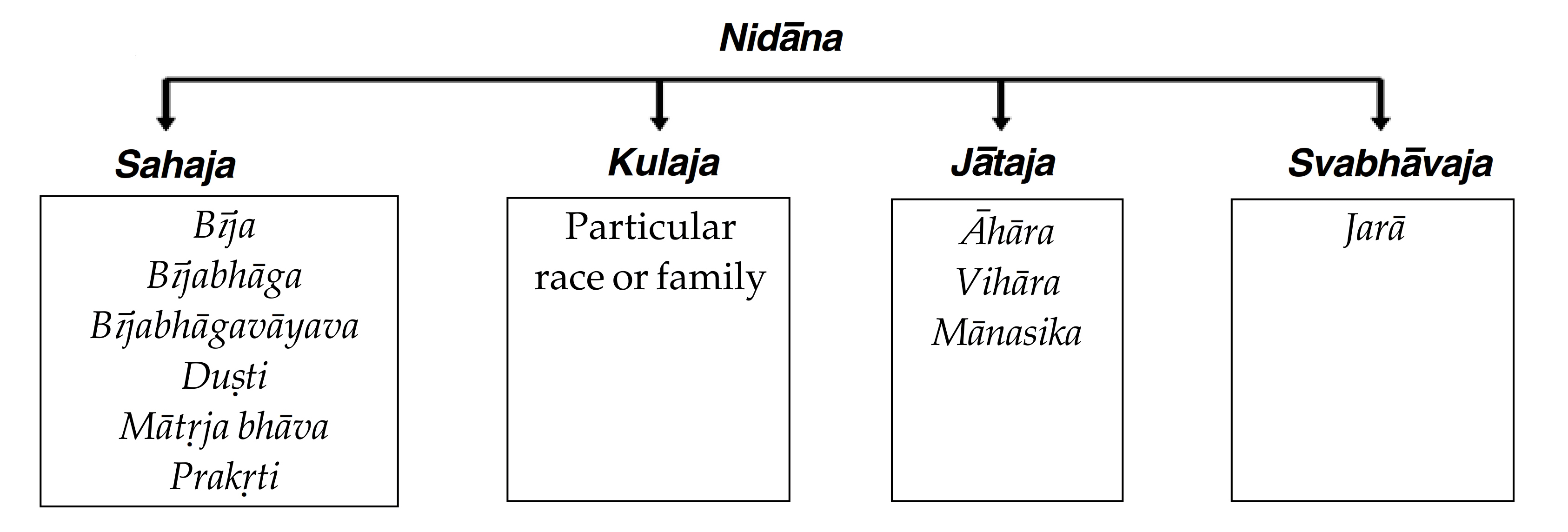
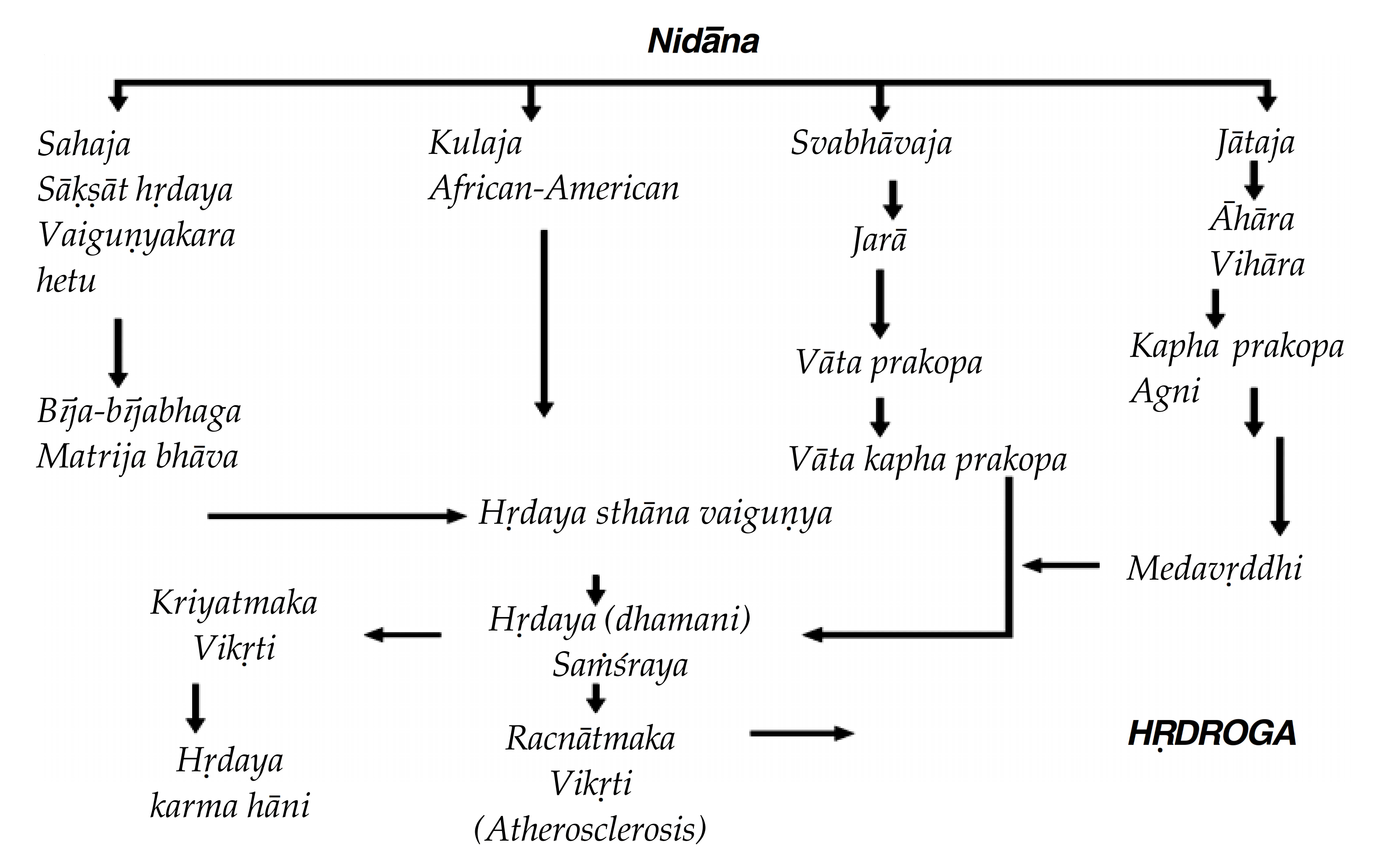
On the page before, is an attempt to classify and depict the etiological causes as sahaja, kulaja, jātaja and svabhāvaja factors. Hereditary causes, the female sex and kaphaja body constitution make a woman susceptible to cardiovascular disease in the later half of her life. Women of Western and African ethnicity can be classified under kulaja factors. Modifiable factors like diet, lifestyle, stress are jātaja factors. Excessive kapha, meda, kleda kara āhāra with less exercise and cintā, etc. are Āyurveda nidāna. Jarā avasthā is an unavoidable factor which causes degenerative changes, especially in women with negative effects of rajonivṛtti which is an important factor.
All the above factors create kapha vāta prakopa with meda duṣti / vṛddhi and getting sthāna saṁśraya in hṛdaya and dhamani, leading to racnātmaka vikṛti (srotorodha), which leads to hṛdroga.
When assessing the clinical picture of cardiovascular disease, i.e. causes, etiopathogenesis, symptoms, CVD in post-menopausal women can be compared with two diseases — kaphaja hṛdroga and medāvṛtta vāta.
Kaphaja hṛdroga
![]()
Bradycardia, heaviness and timidity of the heart, excessive salivation, fever, cough and drowsiness are specific features of the kaphaja type of hṛdroga (13).
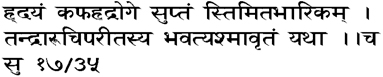
The symptoms of kaphaja heart disease are bradycardia, stiffness, heaviness of the heart, drowsiness and anorexia. The patient feels as if she is loaded with a stone (14).
Medāvṛtta vāta

Occlusion of vāyu by medas (fat) gives rise to the following signs and symptoms:
i. Appearance of oedema in the limbs which is mobile, unctuous, soft and cold; and
ii. Anorexia
iii. This condition is called āḍhya vāta which is difficult to cure (15).
SamprDpti ghattaka
Doṣa — vāta, kapha
Duṣya — rasa, rakta, māṁsa, meda
Srotas — rasavaha, prāṇavaha
Srotoduṣti — saṅga
Agni — jaṭharāgni, dhātu-agni
Treatment
In the kaphaja type of heart disease, treatment should be given after the administration of fomentation, emetic and langhana (fasting therapies) (16).
Shilajatu rasāyana, chyavana prāśa, bramha rasāyana, agastya haritakī or agastya rasāyana, Āmlaka rasāyana are certain formulations mentioned under kaphaja hṛdroga (17).
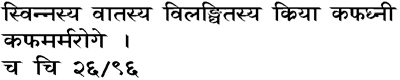
Because of the obstruction to their course by the aggravated vāyu, the medas and kapha get provoked in excess in vāta rakta (gout). In such an event, oleation and roborant therapies should not be employed in the beginning. The provoked fat and kapha should be brought to their normal state by exercise, elimination therapy, the intake of wine and urine, purgation therapy and the administration of buttermilk as well as abhaya (haritakī) (18).
The principle of treatment of cardiovascular disease in post-menopausal women can be considered along the kaphaja hṛdroga and medāvṛtta vāta line of treatment.
Phytoestrogens
Phytoestrogens are plant-derived compounds found in a wide variety of foods, most notably soy. A litany of health benefits, including a lowered risk of osteoporosis, heart disease, breast cancer, and menopausal symptoms, are frequently attributed to phytoestrogens (19).
Role of phytoestrogens in preventing CVD in post-menopausal women
• Reduction of LDL cholesterol and increase in HDL
• Improving arterial elasticity
• Inhibits cell adhesion, alter platelet activating factor and inhibit cell proliferation involved in artherosclerotic lesion formation
• Flax seed — hypercholesterolemia, hypertriglyceridemia, hypertension, atherosclerosis, coronary artery disease
• Use of isoflavones (soy) — beneficial effects on lipids
• Soy protein has been shown in some studies to be able to lower total cholesterol levels by 30% and lower LDL levels by as much as 35-40%.
• Mortality from CHD is less in Japan and this is attributed to the higher content of SOY in the diet (20).
Śatāvari — Asparagus racemosus as a potent phytoestrogen
Śatāvari is a known female rejuvenation mentioned in the Āyurvedic classics as a herb useful for the female reproductive system. The active constituents and its actions based on various researches are as follows:
• Śatāvari — active constituents are steroidal saponins, known as Śatāvarin I to IV.
These are classified under phytoestrogens. Śatāvarin I is the major glycoside with 3 glucose and thamnose moieties attached with sarsapogenin. Śatāvarin IV contains alkaloids, proteins, starch and tannin (21).
• Asparagamine — a polycyclic alkaloid
• Racemosal — a cyclic hydrocarbon
Pharmacological actions
• Anti-tussive , antioxidant
• Immunomodulation — it has an immuneenhancing property by means of enhancing defence functions like leucocytosis and neutrophilia.
• Anti-microbial, cardiotonic
• Oestrogenic — a predominant cornification of epithelial cells have been observed due to presence of oestrogenic activity in Śatāvari
• Polysaccharide and mucilage present in roots
• AR root appears to be useful as a dietary supplement that offers a protection against hyperlipidemia /hypercholesteremia.
• The potent therapeutic phyto-components present in AR root, i.e. phytosterols, saponins, polyphenols, flavonoids and ascorbic acid, could be responsible for increased bile acid production, elimination of excess cholesterol and elevation of hepatic antioxidant status in hypercholesteremic conditions (22).
Discussion and conclusion
The increased incidence of cardiovascular diseases in post-menopausal women and mortality rate due to the same have caused interest in prevention of CVD. This has also led to a tremendous curiosity in herbal alternatives in minimising the risk of diseases such as post-menopausal osteoporosis and heart disease. Research on soy proteins and other phytoestrogens have shown encouraging results in prevention of these diseases. This article is an attempt to understand cardiovascular disease in post-menopausal women under Āyurvedic concepts and to design a special line of treatment and measures to prevent the life-threatening disease. Śatāvari, a known female rejuvenator used for ages for fertility, has shown an effect of minimising the risk of post-menopausal osteoporosis (23). Further research to understand the effect of Śatāvari in preventing cardiovascular disease in post-menopausal women may give encouraging results.
Acknowledgements
We would like to thank Dr. S.K. Khandel, Dr. Rajkumar and Dr. Somraj Kharche for helping us understand the Āyurvedic concepts of this condition.
References
1. Miquel J, Ramírez-Boscá A, Ramírez-Bosca JV, Alperi JD. Menopause: A review on the role of oxygen stress and favorable effects of dietary antioxidants. Arch Gerontol Geriatr. 2006; 42: 289-306. [PubMed]
2. Amin SH, Kuhle CL, Fitzpatrick LA. Comprehensive evaluation of the older woman. Mayo Clin Proc. 2003; 78:1157-85. [PubMed]
3. Applegate W, Blass JP, Williams TF. Instruments for the functional assessment of older patients. N Engl J Med. 1990; 322:1207-14. [PubMed]
4. Gender matters: Heart disease risk in women. Harvard health publications, Harvard Medical school. http://www. health.harvard.edu/newsweek/Gender_matters_Heart_ disease_ risk_in_women.htm [Accessed 17th Sept. 2014].
5. Heart disease kills http://articles.timesof india.indiatimes.com/2011-04- 23/health/28362309_1_heart-disease-coronary-artery-disease-heart-attacks [Accessed 17th Sept. 2014].
6. Unni J. Third consensus meeting of Indian Menopause Society (2008): A Summary. J Midlife Health. 2010 Jan-Jun; 1(1): 43-7.
7. Enas EA, Senthilkumar A, Juturu V, Gupta R. Coronary artery disease in women. Indian Heart J 2001; 53:282-92.
8. NIH conference. Gastrointestinal surgery for severe obesity. Consensus Development Conference Panel. Ann Intern Med 1991; 115(12):956-61.
9. Wassertheil Smoller S et al. Effect of estrogen plus progestin on stroke in postmenopausal women. The women’s Health initiative : a randomized trial, JAMA 2003;289:2673.
10. Grady D et al. Heart and Estrogen Progestin Replacement study follow up (HERS II) 1. Cardiovascular outcomes during 6.8 years of hormone therapy, JAMA 2002; 288:49.
11. Perez Gutthann S et al. Hormone replacement therapy and risk of venous thromboembolism; Population based case control study. BMJ 1997; 314(7084) : 796-800.
12. Thromboembolic accidents in postmenopausal women with adjuvant treatment by Tamoxifen. Bulletin Cancer 1995; 82(1):51-6.
13. Sharma RK, Dash B. Caraka saṁhitā text with English translation and critical exposition. Vol. 4. Varanasi: Chaukhambha Sanskrit Series Office; 2009, p. 492.
14. Sharma RK, Dash B. Caraka saṁhitā text with English translation and critical exposition. Vol. 1. Varanasi: Chaukhambha Sanskrit Series Office; 2004, p. 316.
15. Sharma RK, Dash B. Caraka saṁhitā text with English translation and critical exposition. Vol. 5. Varanasi: Chaukhambha Sanskrit Series Office; 2010, pp. 38-9.
16. Sharma RK, Dash B. Caraka saṁhitā text with English translation and critical exposition. Vol 4. Varanasi: Chaukhambha Sanskrit Series Office; 2009, p. 496.
17. Acharya YJT. Caraka saṁhitā with Commentary by Chakrapani. 5th Edition. Varanasi: Chaukhambha Sanskrit Bhavan; 2001. pp. 377-8.
18. Sharma RK, Dash B. Caraka saṁhitā text with English translation and critical exposition. Vol. 5. Varanasi: Chaukhambha Sanskrit Series Office; 2010, p.126.
19. Patisaul H, Jefferson W. The pros and cons of phytoestrogens. Front Neuroendrocrinol. 2010; 31(4): 400-14.
20. Kritz-Silverstein, D, Goodman-Gruen, DL. Usual dietary isoflavone intake, bone mineral density, and bone metabolism in post-menopausal women. Journal of Women’s Health and Gender-Based Medicine 2002; 11: 69-78.
21. Negi JS. et al. Chemical constituents of Asparagus. Pharmacognosy Reviews 2010; 4 (8): 215-20.
22. Visavadiya NP, Narasimhacharya AV. Hypolipidemic and antioxidant activity of Asaparagus racemosus in hyperchol-esteremic rats. Indian Journal of Pharmacology 2004; 37(6): 376-80.
23. Japee J, Pandya M. A comparative study on shatavari and kukkutanda twak bhasma in minimizing the risk of postmenopausal osteoporosis. AYU 2009; 30(3): 314-7.
Glossary of Āyurvedic terms
Agastya haritakī — an Āyurvedic compound preparation.
Agastya rasāyana — an Āyurvedic compound preparation.
Āmlaka rasāyana — an Āyurvedic compound preparation.
Bīja — seed. It is the term used for denoting sperm and ovum in Āyurvedic literature. Reproductive element.
Bījabhāga — chromosomes.
Bījabhāgāvayava — genes.
Bramha rasāyana — an Āyurvedic compound preparation.
Chyavana prāśa — an Āyurvedic compound preparation.
Cintā — worrying.
Dhamani — an artery, or all channels circulating blood.
Dhātu — tissues, Seven dhātus mentioned in Āyurveda
Dhātu-agni — tissue agnis; there are seven, one for each of the major tissues of the body.
Doṣa — three main forces which govern the body (vāta, pitta and kapha); literally means faulty or to cause harm, although they only do so when they are functioning abnormally. When functioning normally, they maintain good health of the body and guide all of the normal bodily functions.
Duṣti — Unhappiness. It is also used for abnormality in the doṣas and dhātus.
Duṣya — termed for dhātus which are vitiated by doṣa.
Hṛdaya — heart.
Hṛdaya karma hāni — loss of heart function.
Hṛdroga — heart disease.
Jarā — old age
Jātaja — acquired factor for disease.
Jaṭharāgni — the digestive fire; the most important of all the agnis. Also called kayagni (bodily fire) and antaragni (internal fire).
Kapha — one of the three doṣas in the body. The force behind the structure and stability of the body; the elements are water and earth; its qualities are heavy, cold, moist, static, smooth and soft; its root is in the upper stomach. Also a term for mucous.
Kleda — with too much moisture.
Kulaja — genetic factor for disease.
Māṁsa dhātu — one of the seven dhātus or tissues; consists of muscles, ligaments and skin. Composed mainly of earth and some water and fire.
Mānasika — psychological.
Mātṛja bhāva — maternal factors. One of the six factors responsible for genesis.
Meda dhātu — one of the seven dhātus or tissues; consists of fat (composed primarily of water). Lubricates tissues of body through oiliness.
Medāvṛtta vāta — a condition caused by obstruction of vāyu doṣa by abnormal meda dhātu.
Nidāna — causative factors.
Prakopa — vitiation of doṣa. Prakopa is described as a second stage in the patho-genesis of any disease.
Prakṛti — personality, Pure potential for matter (unmanifested potential); the soul's guna (sattva, rajas or tamas) in its seed form.
Prāṇavaha srotas — the channel that carries prāṇa; usually refers to the respiratory system (nasal passages, sinuses, bronchi and lungs); also relates to the colon which, through the process of digestion, also extracts and absorbs a large amount of prāṇa; originates in the heart.
Racnātmaka vikṛti — anatomical/structural deformity.
Rajonivṛtti — cessation of menstruation — menopause.
Rakta dhātu — one of the seven dhātus or tissues; consists of blood/ red blood cells. Also involves blood vessels, liver and spleen. It contains the fire element; invigorates tissues and the mind.
Rasa dhātu — one of the seven dhätus or tissues; consists of all bodily fluids (plasma, lymph, chyle, breast milk, menses). In the subtle body, it provides a sense of satisfaction.
Rasavaha srotas — the channel through which aahaara rasa flows; originates in the heart and blood vessels and includes lymphatic vessels; primary carrier of kapha doṣa.
Sahaja — congenital factor for disease.
Samprāpti — etiology.
Samprāpti ghaṭaka — elements involved in pathogenesis of disease.
Saṁśraya — taking shelter at a particular location.
Saṅga — obstruction.
Shilājatu rasāyana — Āyurvedic compound preparation.
Srotas — channels in the body; some are gross and some are subtle. In some texts, srota is used synonymously with nadī. The ears are also called srota.
Sroto rodha — obstruction of channels.
Sthāna saṁśraya — accumulation of vitiated doṣas in a susceptible channel of the body.
Svabhāvaja — natural causes.
Vaiguṇya — deformity, abnormality.
Vaiguṇyakara hetu — factors causing abnormality.
Vāta — One of the three doṣas. The force within the body responsible for all motion; its elements are air and ether; its qualities are light, cold, dry, mobile, subtle and rough; its root is the large intestine.
Vāyu — one of the three doṣas. The force within the body responsible for all motion; its elements are air and ether; its qualities are light, cold, dry, mobile, subtle and rough; its root is the large intestine.
Vihāra — regimen, routine, conduct.
Vikṛti — abnormality, vitiation.
Vṛddhi — increase.
1 heart attack
Dr. Jasmine Gujarathi is Associate Professor at Dept. of Prasuti Tantra and Stri Roga; Dr. Ritesh Gujarathi is Associate Professor at Dept. of Basic Principles, G. J. Patel Institute of Ayurvedic Studies and Research, New Vallabh Vidyanagar, Anand, Gujarat.
Share with us (Comments,contributions,opinions)
When reproducing this feature, please credit NAMAH,and give the byline. Please send us cuttings.









