Homoeopathy
Clinical evaluation of Trombidium in amoebic dysentery
Editor’s note
Amoebic dysentery is a common intestinal infection in the Indian context. While allopathic treatment is quite effective at controlling it in the acute stages, it is difficult to completely eradicate the organism from the intestine as it burrows deep inside, making it difficult for allopathic drugs to reach. In a first of its kind study, we find that the homoeopathic drug Trombidium is quite effective in treating the infection in the acute phase. This opens doors to further possibilities of experimenting with the efficacy of the drug in chronic amoebic colitis, especially since homoeopathic medication acts through other modalities than the conventional allopathic medication. Given the positive results of the study being presented here, we hope that further research will be undertaken along these lines in chronic conditions where there are very few options in modern medicine. What makes this study interesting though, is that stringent criteria consistent with the scientific temper of the times have been used in assessing the efficacy. This assuages the common charge levied against homoeopathic medicine by the allopaths that it is merely faith healing with little basis in scientific medicine!
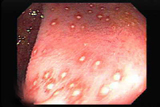
Amoebic dysentery is caused by Entamoeba histolytica, a potentially pathogenic intestinal amoeba that is propagated among humans by its cysts, 10 micron or more in diameter. Entamoeba histolytica must be distinguished from other species which are non-pathogenic and exist as commensals in the intestine, notably Entamoeba hartmanii and Entamoeba coli. Amoebic dysentery is endemic in many tropical countries and it commonly spreads by water or contaminated uncooked food, especially raw vegetables and salads. Flies may also carry the cysts and spread the amoeba from the faeces of infected persons to food.
Amoebic dysentery is characterised by frequent passage of small amount of watery stools, often containing blood and mucus, accompanied by severe abdominal cramps. Ulceration of the walls of the large intestine may occur. There may be tenderness along the line of the colon, usually more marked over the caecum and pelvic colon.
Symptomatic acute amoebic colitis develops after 2 to 5 days of an incubation period, but it may take longer also. Abrupt onsets of diarrhoea with mucus and blood in the stools, a grumbling and cramping pain in the abdomen are almost always diagnostic features of amoebic dysentery. Less than 40% of patients with amoebic dysentery may be mildly febrile.
Abundant references of homoeopathic medicines found useful in diarrhoea and dysentery simulating intestinal amoebiasis are available in literature. However, no pathological confirmation is cited anywhere.
The hypothesis was that certain lesser known/partially proved homoeopathic drugs that are mentioned in the literature for diarrhoea and dysentery have close resemblance to acute intestinal amoebiasis. Fragmented references of these drugs exist in homoeopathic literature for intestinal conditions like diarrhoea and dysentery, but there is no reference to amoebiasis or amoebic dysentery.
This is a study undertaken at Sonajirao Khsirsagar Homoeopathic Medical College & Hospital, Beed, where a good number of cases of amoebic dysentery were observed. We designed this study to evaluate the efficacy of Trombidium, a lesser-known medicine for amoebic dysentery in the management of this disease.
Aims and objectives
The objective of the study was to evaluate the efficacy of Trombidium in the treatment of Amoebic dysentery.
Material and methods
Cases of different age-groups were enrolled into the study. All were patients attending the OPD of S.K. Homoeopathic Medical College & Hospital, Beed, fulfilling the inclusion criteria given below. They were screened and confirmed with the indication of Trombidium, as given in Table 1. Of those screened, patients who came within the domain of symptomatology of Trombidium were enrolled in the study. Data of all enrolled patients is given in Table 2.
Cases were diagnosed on the basis of subjective and objective symptoms. Cases with different duration of complaints were also enrolled for the study. The basis for prescription for these cases was presenting signs and symptoms.
Inclusion criteria
Patients were screened at the OPDs. Those who fulfilled the following criteria of subjective and objective symptoms were registered in the study:
• Frequent diarrhoeal stools and/or
• Stools with mucus and blood
• Tenesmus associated with stools and/or
• Grumbling, cramping pain in the abdomen
• Pyrexia may or may not be present.
Exclusion criteria
Severe cases warranting hospitalisation were excluded from the study.
The case history of each subject was recorded in detail. A clinical diagnosis was made on the basis of above referred symptoms and signs. Medicine was prescribed on the symptoms and signs of Trombidium as given in Table 1. Help was taken from the Repertory.
The dosage, potency and repetition of the drugs were determined as per homoeopathic principles, taking into consideration the presentation of each individual case.
Assessment criteria
The improvement assessment was done on the following symptoms/signs:
• Frequency of stools: reduction in or restoration to normal.
• Improvement in or disappearance of pain and tenesmus.
• Disappearance of blood and mucus from stools.
• Relief in pyrexia, if present.
Pre-defined criteria, as detailed in Table 3, were followed for assessment of treatment after treatment.
Table 1: Indication for prescription of Trombidium
• Dysentery, agg. by food and drink
• Pain in rectum before and after stool
• Griping pain and tenderness in abdomen
• Stools loose, watery, mixed with blood and mucus
• Burning at the anus
Table 2: Details of patients enrolled in the study
No. of patients |
|
| No. of screened patients | 1104 |
| No. of enrolled patients | 200 |
| No. of drop out patients | 18 |
| Total no. of patients assessed | 182 |
Table 3: Parameters adopted for assessment of improvement after treatment
| Post-treatment outcome | Criteria for assessment |
| Cured | Complete removal of subjective & objective symptoms with no subsequent recurrence for a period of 1 year. |
| Improvement marked | Complete removal of subjective and objective symptoms except occasional recurrence of attacks. |
| Moderate | Subsidence of subjective and objective symptoms with decrease in duration, intensity and frequency of attacks. |
| Mild | Partial relief of subjective and objective symptoms. |
| No improvement | No response after considerable period of treatment. |
| Worse | Despite treatment, disease worsens and complications arise. |
| Not reported | Patient does not report back after first or second visit. |
| Dropped out | Poor compliance by the patient as to specific treatment and management. |
Results
Improvement of all the cases was assessed after treatment on the basis of pre-defined criteria given in Table 2. Patients were followed up for varying periods. Improvement in the symptoms are presented in Table 4.
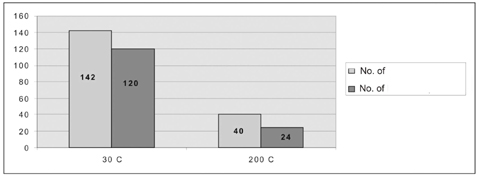
In 142 cases, 30C potency was used, whereas in 40 cases 200C potency was used. Cases where 30C potency was used showed better results, whereas cases with 200C yielded less favourable results. Results of potency-wise improvement is given in Table 5.
Table 4: Improvement in symptoms after treatment
| No. of patients | |||
| Before treatment | After treatment | Improved | |
| Frequency of stools increased |
162 | 42 | 120 |
| Mucoid stools | 102 | 18 | 84 |
| Bloody stools | 124 | 48 | 76 |
| Tenesmus | 140 | 11 | 129 |
| Flatulence | 82 | 17 | 65 |
| Pyrexia | 42 | 4 | 38 |
Fig 1: Improvement in symptoms after treatment
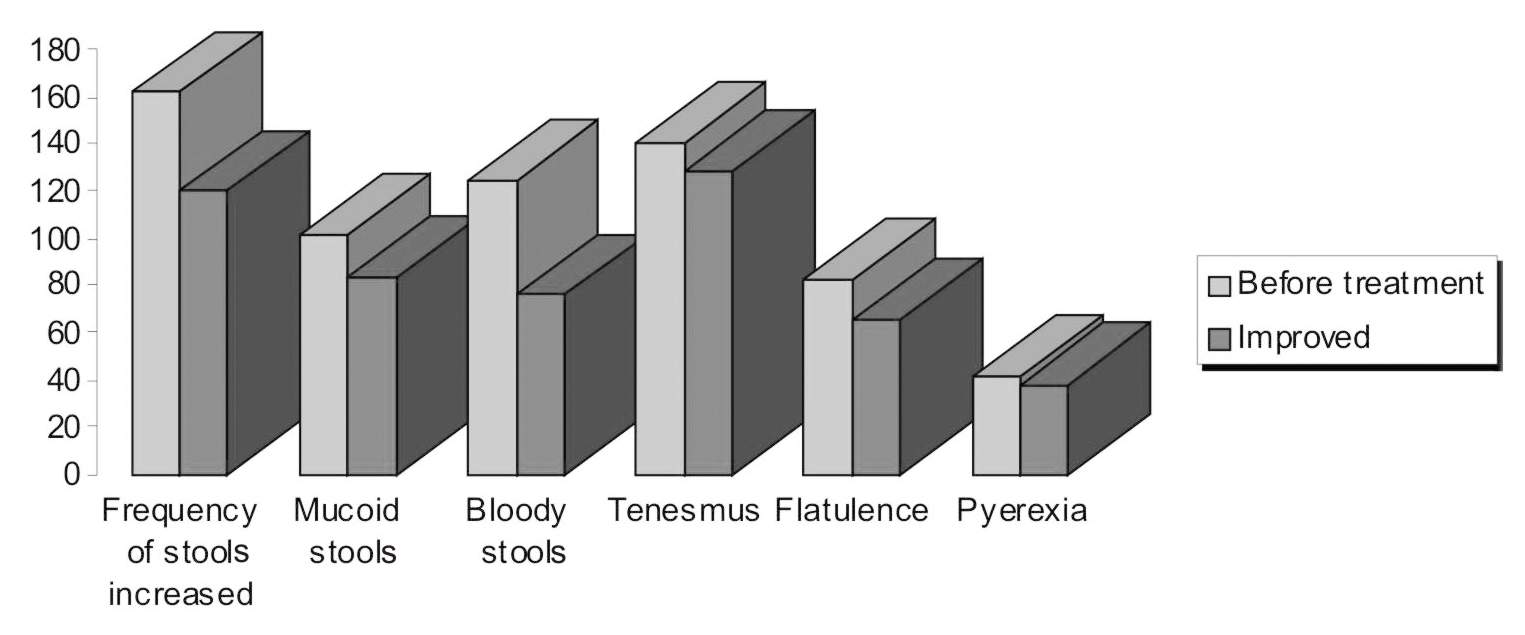
Table 5: Potency-wise improvement
| No. of patients | ||
| Prescribed | Improved | |
| 30 C | 142 | 120 |
| 200 C | 40 | 24 |
Fig 2: Potency-wise improvement
Discussion
Trombidium was found to be very effective in the management of amoebic dysentery. These medicines were used in 30 and 200 potencies. Trombidium was more useful when prescribed in 30C potency.
Trombidium was found to be more effective when patients had presented with mucoid stools and tenesmus, but was less effective with bloody stools. Frequency of stools was increased in 162 patients before treatment, but after treatment 120 patients improved. Mucoid stools were present in 102 patients before treatment and improved in 84 patients after treatment. Bloody stools were present in 124 patients before treatment and improved in 76 patients after treatment. Tenesmus was present in 140 patients before treatment and after treatment it improved in 129 patients. Flatulence was present in 82 patients before treatment and after treatment it improved in 65 patients. Pyrexia was present in 42 patients before treatment and after treatment it improved in 38 patients.
After studying an adequate sample size, inferences are derived from the data collected during the study. From this study it is evident that rare and lesser-known drugs can be of great use, if their potential is explored by undertaking such clinical trials in a phased manner.
This is evident from the fact that a good number of patients were screened in order to have a proper sample size in the study. All those screened were provided free medical treatment for whatever disease they were suffering from.
Notwithstanding the constraints at various levels, especially non-availability of investigation facilities required for the project, the results of this study are statistically valid and indicate a positive role of the lesser- known drug, Trombidium in the treatment of amoebic dysentery. However, any shortcomings of this clinical trial can be overcome by under-taking a further study with laboratory investigation facilities at every study centre.
Conclusion
Thus, the objective of the study to evaluate the efficacy of Trombidium in amoebic dysentery is achieved. Due to lack of laboratory facilities, the efficacy of the drugs could not be corroborated with laboratory findings. The corroboration of symptoms of this medicine with those given in the Materia Medica confirms the patho-genesis of this lesser-known drug and reaffirms its therapeutic potential.
Dr. Arun Bhasme is the Principal of Sonajirao Kshirsagar Homoeopathic Medical College & Hospital, Beed (M.S.).
Share with us (Comments, contributions, opinions)
When reproducing this feature, please credit NAMAH, and give the byline. Please send us cuttings.