The body
Healthy bowel habits
Abstract
The state of a cleared bowel movement is a great relief for everyone. One should pass regular bowel movements without straining or using laxatives. The faeces in normal course are soft yet well-formed, easily passed and at a frequency anywhere between 1–3 times a day and 3 times a week. It is not absolutely essential for one to have it each day. One should promptly comply with the urge to defecate. If it is not heeded within a few minutes, the urge usually passes off. It may take just one or two minutes to accomplish the defecation. The postures and modalities of defecation are culture-dependent. Faeces contain 65-85% water. Constipation, being a common problem, might result in hard, dry faeces that are difficult to pass. If defecation occurs too fast, before excess liquid is absorbed, it gives rise to diarrhoea. Innumerable disease conditions are diagnosed based on bowel symptoms. Intake of high fibre foods, drinking plenty of water; not straining for stools, complying promptly with the urge to pass stools and optimum physical exercise are the best means to prevent bowel-related diseases.
A bowel movement (defecation) is the act of eliminating solid or semi-solid waste materials (faeces) from the digestive tract. A state of cleared bowel movement is a great relief for everyone. It is common to have a bowel movement once every day and that too in the morning hours. However, the normal frequency of bowel movement is from three times a day to three times a week. It is not absolutely essential for one to have it each day but one should be able to pass regular bowel movements without straining or using laxatives. The faeces in a normal course are soft yet well-formed, easily passed and at a frequency anywhere between 1–3 times a day and 3 times a week.
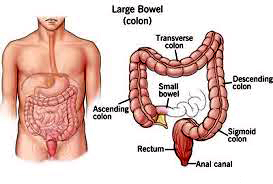
Anatomy and physiology of bowel movement
The rectum is a distensible muscular tubular space acting as a temporary storage space for excrement (faeces).Muscular contractions (rhythmic peristaltic wave-like movements) in the walls of the colon move faecal material through the digestive tract to the rectum.When the rectum is moderately filled, pressure within it is increased. This pressure stimulates the urge to defecate. This increased intra-rectal pressure initially forces the walls of the anal sphincter apart and allows excretion of the faecal material through the anal outlet. The muscles attached to the pelvic floor further help to pull the anal sphincter apart. The rectum shortens by contraction of circular muscles in order to expel material into the anal outlet. The peristaltic waves propel the faeces out of the rectum. In the anus there are two muscular constrictors, the internal and external sphincters that govern the passage of faeces or retention of faeces. As the faeces form, the anus is drawn up over the passing mass by muscles of the pelvic diaphragm to prevent prolapse of the anal canal.While defecation is occurring, the excretion of urine is usually stimulated. Once defecation is complete, the space of the rectum undergoes involution.
One should promptly comply with the urge to defecate. If it is not complied by within a few minutes the urge passes off. This leads to the return of the faeces back to the colon. Under these circumstances, returned faeces may get hardened by further absorption of water in the colon. If defecation is delayed for a prolonged period the faecal matter may harden, resulting in constipation.
Some people cultivate a wrong habit of defecation by straining. During the act of straining the lungs push the diaphragm down to exert the pressure. If one strains hard to facilitate excretion, the chest muscles, diaphragm, abdominal-wall muscles and pelvic diaphragm all exert intra-abdominal pressure. Respiration temporarily halts as the filled lungs push the diaphragm down to exert pressure. It can give rise to prolapse of the rectum. It can aggravate inguinal hernia. The straining to defecate also results in the rising of blood pressure. Such excessive straining for defecation can be hazardous to health. It can cause cardiac arrest and other cardiovascular complications.
In healthy bowel movement conditions, one gets well-formed faeces. It may take just one or two minutes to accomplish the defecation. The postures and modalities of defecation are culture-dependent. Squatting toilets are used by the vast majority in India.There would be no irritation. In ideal cases there would be no trace of faecal matter smeared on the outer anal skin or buttocks. In general the anus and buttocks need to be cleansed after defecation. In India,water is used for anal cleansing after defecation (exclusively or in addition to using toilet paper).
Water consumed by us orally gets completely absorbed in the small and large intestines. Faeces contain 65-85% water. The cellulose component of food is completely indigestible fibre, providing volume and bulk to the faeces. The more fibre one eats the more of undigested food wastes can be discharged from the body. The normal colour of faeces should be brownish in adults and yellow in infants. White or clay-coloured faeces indicate a block of the bile duct, obstructing the passage of bile in the system. Black tarry faeces indicate bleeding in the gastrointestinal tract or consumption of iron supplements. Bright red-coloured blood indicates bleeding in lower gastrointestinal tract (rectum or near the rectum). The normal shape of faeces is cylindrical, about 2.5 cm in diameter in adults. The normal amount emitted per day would be between 100 to 400 grams per day depending upon the person’s diet. Normal odour: aromatic, affected by ingested food and person’s own bacterial flora. In teething children, the odour of faeces may emit a strong sour smell.
Quality of healthy bowel habits
1. Able to hold on for some time following the urge to go to the toilet till one gets acomfortable place to defecate. However, one should never ignore the urge to have a bowel movement.
2. Able to pass a bowel motion within about a minute or two after sitting down on the toilet seat.
3. Able to pass a bowel motion without even the slightest strain or struggle.
4. Have an absolutely cleared feeling after one passes motion.
5. Faeces are soft yet well-formed. You can consider faeces well-formed when they settle at the bottom of a water column in the commode and the water around the faeces is clear.
Common clinical conditions related to bowels
Constipation
A common problem might result in hard, dry faeces that are difficult to pass. It can be caused by a faulty lifestyle like non-consumption of a fibre-rich diet, lack of physical exercise and less consumption of fluids leading to dehydration. Drinking adequate water before each meal will result in maintaining good hydration. Functional constipation is a bowel disorder that presents as persistently difficult, infrequent or seemingly incomplete defecation. It is estimated to affect one-third of the people in a population with a sedentary lifestyle. There are instances where a person with constipated feelings uses his own fingers to help empty the bowel, either by performing a manual evacuation of the faeces or supporting the perineum. Many physicians advise people to rise early in the morning and consume copious quantities of warm water. Drinking warm water in the morning on waking facilitates easy evacuation of faeces.
There should be enough fibre in one’s diet to ensure that faeces are soft and pass painlessly and easily. Constipation can be one of the indications of hypothyroidism or aluminium poisoning. Chronic constipation could lead to other complications. Straining to pass faeces could lead to the development of haemorrhoids, rectal prolapse or anal fissure. Dry hard faeces can cause faecal impaction, leading to intestinal obstruction.
Diarrhoea
A common condition in which the patient passes watery faeces more than three times a day. In case of diarrhoea, the water content of faeces is more than 85%. Prolonged diarrhoea can cause severe dehydration requiring emergency care. Chronic diarrhoea can be an indication of disorders like hyperthyroidism and irritable bowel syndrome. One should drink lots of fluids to overcome the dehydration caused by diarrhoea. Diarrhoea or abnormally frequent defecation is a characteristic symptom of many diseases and disorders. If defecation occurs too fast, before excess liquid is absorbed, diarrhoea is the result.
Incontinence
Faecal incontinence (FI) in adults is estimated to affect 2% of the population.The incidence of anal incontinence is grossly underestimated because of under-reporting. Many have combined urinary and faecal incontinence. Physiologically the bowel movement is under voluntary control. Young children learn voluntary control through the process of toilet training. The anal and urethral sphincter muscles are closely linked. This explains why defecation is frequently accompanied by urination. There are possibilities of developing incontinence. It may develop with age. It may also come as aresult of surgical, obstetric, spinal or other bodily injuries. It may also be an effect of neurological impairment secondary to diabetes, cerebral-vascular accidents or multiple sclerosis. Incontinence may also be influenced by pain, fear, temperature elevation and psychological or neurological complications.
Haemorrhoids
Haemorrhoids are very common. It is estimated that 75% of the adult population will have haemorrhoids at some point of their lives. Sometimes they don’t cause any symptoms but at other times they can cause itching, discomfort and bleeding as a result of engorgement of the rectal veins. The habit of straining for defaecation might aggravate bleeding from haemorrhoids.Haemorrhoids are more likely with aging because the tissues that support the veins in your rectum and anus can weaken and stretch. The haemorrhoids may bleed while defecating, some may just protrude. Occasionally they get thrombosed, making it avery painful condition.
There are innumerable disease conditions which have their indication in bowel dysfunctions. I remember a middle-aged lady who was being treated for amoebic colitis for more than six months. She used to get frequent dysenteric stools, scanty with mucus and tenesmus. Coincidently her faecal examination revealed presence of Entamoebahistolyticacysts. She was asked to consume only boiled water. They pumped antiprotozoal medicines into her with no relief. Symptoms like low-grade fever, loss of weight and palpitations prompted me to check her thyroid profile. It clearly indicated thyrotoxicosis. Once her thyroid functioning was moderated with anti-hyperthyroidism agents (neomercazole) her so-called amoebic colitis got cured. It was her thyrotoxicosis which was causing frequent bowel motions and not amoebiasis.
Another lady had prolapse per rectum. She was having inactive rectum with no urge for defecation. It was a great task for her to clear the bowels. She was almost dependent upon laxatives for clearing her bowels. The presence of complaints like rectal sluggishness, intolerance to cold and weight gain prompted us to study her thyroid profile, which showed she was in a hypothyroid state. Mere thyroid supplements and pelvicfloor exercises helped her to get rid of her complaints.
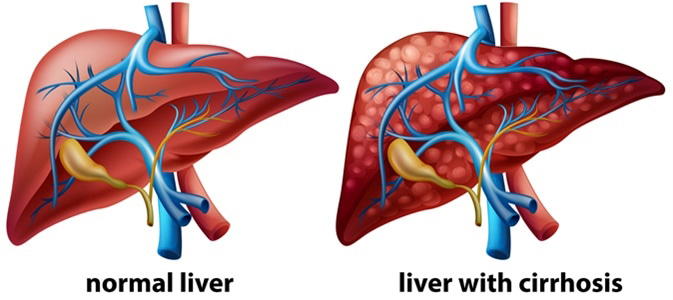
In many instances, haemorrhoids can be indicators of cirrhosis of the liver as rectal veins are a site for shunting of systemic and portal circulation.
I once treated one boy aged 12 years for faecal incontinence. He used to get sensations of passing flatus during which faeces used to escape. His parents and teachers used to reprimand him for his incontinence. He was reluctant to attend school for this reason. It took three months to treat him with due counselling and homoeopathic medicines.
A girl with hepatitis A had white faeces while icterus (yellow discoloration of skin and sclera) was apparent all over. When treatment was started for the liver infection the girl started getting yellow faeces, which is a sign of regression of inflammation in the liver. It indicates that the obstruction to the flow of bile had been released with regression in the swelling or congestion of the liver. This is the reason why we clinicians enquire about thecolour of stools.
Prevention of bowel related diseases
The best way to prevent bowel-related disorders is to keep your stools soft, so they pass easily.
1. Eat high-fibre foods: eat more fruits, vegetables and whole grains. Doing so softens the stool and increases its bulk, which will help you avoid any straining. On an average each day, one should consume 35 to 40 grams of cellulose containing fruits and vegetables.
2. Drink plenty of fluids: drink ample water in a proper pattern. It is beneficial to drink fluids to the tune of one litre before each of the three meals (breakfast, lunch and dinner). This will help to keep the faeces soft.
3. Don’t strain: straining and holding your breath when trying to pass stool creates greater pressure in the veins in the lower rectum.
4. Comply with the urge promptly as soon as you feel it: if you delay the urge to pass a bowel movement it may cease and faeces could become dry and be harder to pass.
5. Exercise: staying physically active in general helps one to have healthy bowel movements.
6. Adequate sleep: timely sleep (midnight being mid-point) for adequate duration directly and indirectly helps in maintaining a healthy bowel movement.Dr. Uttareshwar Pachegaonkar and Dr. Arati Sharma are both Directors at the Sri Aurobindo Centre for Homoeopathy, Sri Aurobindo Society at Pondicherry.
Share with us (Comments,contributions,opinions)
When reproducing this feature, please credit NAMAH,and give the byline. Please send us cuttings.