Surgery
A review of kṣārasūtra management in high anal fistula
Editor's note
There is a growing general consensus that ancient India had its own fairly developed system of science, mathematics, medicine and even surgery. Still, most textbooks, when they describe the evolutionary history of medicine depict everything other than the modern allopathic system as primitive early explorations. This condescending attitude has done much harm to modern medicine, since it neither tries to understand nor utilise the wide experience and intuitive knowledge of those who have gone before us. This article however throws a fresh insight and compares an ancient surgical technique for treating ano-rectal fistula with present-day surgical options. It is a difficult task and yet the author does it well. It is almost as if Suśruta were present in our own time discussing his methods in a modern medical forum!
Introduction
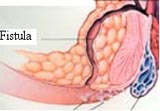
This disease, high anal fistula, a common ano-rectal disorder which usually results as a sequel to some varieties of ano-rectal abscesses, is as old as mankind and a challenge to surgeons even today. Fistula-in-ano has been recognised as a distinct entity for thousands of years. In the fifth century B.C., Hippocrates advocated the laying open of fistulas, including complex fistulas. One would think that after 2,500 years the controversies in the management of fistula-in-ano would have been resolved. But this is not the case and much about the management of fistula-in-ano is still being debated. Available surgical procedures may not only result in incontinence but also recurrences. They cause discomfort and absence from work with the consequent economic strain.
Keeping these problems in mind, Susturta (800 B.C) has described the kṣārasūtra technique whereby a medicated alkaline thread, impregnated with the paste of Curcuma longa and latex of Euphorbia rerifolia, is employed along the fistula track which cuts itself and heals the wound naturally from inside (1). However, here are a few questions which need to be addressed to make this technique relevant in the present scenario:
• Where and when should an abscess be drained? Can kṣārasūtra be appliedimmediately after drainage?
• Should a primary fistulotomy be performed before the kṣārasūtra application?
• What pre-operative evaluation is essential for preventing recurrences and other complications?
• Should a simple fistula be managed by fistulectomy or fistulotomy?
• Does kṣārasūtra also prove to be the best technique for the management of complex fistulae?
1. Where and when should an abscess be drained? Can kṣārasūtra be applied immediately after drainage?
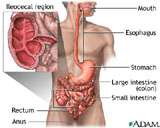
The crypto glandular nature of fistula-in-ano is now generally accepted. Eisenhammer coined the term ‘fistulous abscess’ to denote the continuum between the stage of acute abscess and chronic fistula-in-ano. An abscess can be classified as peri-anal, intra-muscular, ischio-rectal or supra-levetor. With the exception of supra-levetor and some intra-muscular abscesses, most can be managed in the clinic under local anesthesia. A cruciate incision is made as close to the anal canal as possible without damaging the external anal sphincter. The skin edges are trimmed to promote adequate drainage, and haemostasis is achieved using electrocautery. There is no need to aggressively break the loculations as they spontaneously rupture and drain into the cavity. Antibiotics may not be necessary until and unless there is a massive peri-anal abscess. Those in favour of primary fistulotomy argue that it eradicates the infection process, thereby eliminating or reducing the incidence of recurrent abscess or fistula formation. Those against primary fistulotomy point to the difficulty in identifying the fistula tract and primary opening in the setting in of acute inflammation. Overzealous probing may result in the formation of a false tract, which makes it difficult to manage supra or extrasphincteric fistula (2). In addition, proponents of delayed fistulotomy argue that acute ano-rectal suppuration will not inevitably lead to the formation of fistula-in -ano.
kṣārasūtra application at this stage, without finding the exact internal opening, is a futile exercise. But recurrent drainages will probably have internal openings: in such conditions kṣārasūtra application may be useful and successful.
2. Should a primary fistulotomy be performed before kṣārasūtra application?
Controversy exists as to whether an immediate fistulotomy be performed before kṣārasūtra application. Those in favour of primary fistulotomy argue that it eradicates the infectious process, thereby eliminating or reducing the incidence of recurrence. Moreover it drains all the infectious material very fast, thus minimising post-operative pain (3).
Nearly 60 percent of those patients treated with partial fistulotomy with kṣārasūtra application were spared repeated fistulotomy (4). Disturbances in continence were found in some cases apart from heavy bleeding and a big wound. Higher antibiotics are essential in the post-operative period. Primary fistulotomy, except in rare instances, should be discouraged.
3. What pre-operative evaluation is essential for preventing recurrences and other complications?
A careful history and physical examination are crucial in the evaluation of the patient with a chronic fistula-in-ano. A focused history regarding gastrointestinal symptoms, diarrhoea, previous ano-rectal surgery, and prior history of any ano-rectal abscess is taken. Careful examination for stigmata of peri-anal Crohn’s disease should be done, including lateral fissures, hypertrophied skin tags, and anal stenosis. Sigmoidoscopy is routinely performed at the time of fistulotomy, but in the absence of significant history or physical findings, it is not necessary to aggressively rule out Crohn’s disease (5).
Tools currently available include fistulography, sonography, magnetic resonance imaging and manometers. All biophysical evaluations have their role in assessing the internal sphincter from the anal mucus and ultrasonography in the evaluation of the pathology in the ischio-rectal fossa and in the evaluation of supra-anal infra-levator extensions. However, these procedures have the disadvantage of being expensive and are not uniformly available (6).
The goals of surgery for fistula-in-ano are the eradication of infection and prevention of recurrence while minimising disturbances of fecal continence. A retrospective study of 975 high anal fistula cases with kṣārasūtra application to study the associated factors revealed that the majority had true high anal fistulae, horse-shaped extension and some even did not have an internal opening. Previous fistula surgery was also a factor associated with recurrences.
4. Does kṣārasūtra also prove to be the best technique for the management of complex fistulae?
Several techniques are available to treat a patient with a fistula. However, modern surgical procedures like fistulotomy or fistulector my not only result in recurrence but also cause a number of complications like stenosis, retention of urine, sphincteric incontinence. Discomfort, surgery induced weakness and economic strain are additional disadvantages. These surgical processes require patients to undergo painful operative and post-operative procedures and can also result in incontinence. Treatment should always be a balance between curing the inflammatory process and preservation of the sphincter function. (7)
More complex fistulas like high anal fistula, horseshoe extension or fistulas in high-risk situations, especially in female patients with anterior fistulas, require investigation before treatment in order to decrease complications of incontinence or non-healing. We have not found fistulography to be helpful for these fistulas. However, ultrasound and MRI can certainly provide important information about anatomy and identify multiple tracts and occult small abscesses. These tests are particularly important in the recurrence of poorly draining fistula or in situations where the patient has symptoms of pain and intermittent drainage although no fistula tract can be identified (8).
Keeping all these problems in mind, there is a new approach of kṣārasūtra which is employed after probing the track with a malleable probe and holding the thread in the sphincter bundle. Because of its kṣaṇana (burning) and kṣaraṇa (cutting) properties, the thread cuts the track from inside gradually and allows for simultaneous healing. In this, the cutting property may be attributed to the alkaline nature of the thread and the healing property may be attributed to the turmeric powder and the latex of Euphorbia nerifolia (9).This less extensive surgical procedure does not disturb the sphincter bundle, thus safeguarding the sphincter tone and preventing post-operative incontinence. The kṣārasūtra holds the major track and allows the other minor track to drain and heal spon-taneously given sufficient time and scope. This can destroy the cryptic material of the track and prevent recurrence. It does a chemical fistulectomy and averts incontinence. The efficacy of the treatment is measured with UCT (unit cutting time). The correlation between the length of the track and duration of treatment is statistically significant (10).
Conclusion
Anal disease, although a common cause of morbidity in the general population, is often poorly understood and managed by medical students, general practitioners and surgical trainees. Surgical residents frequently fail to grasp the finer details required by anal surgery, considering it not particularly exciting compared to other more prominent procedures. Acute ano-rectal abscess and fistula-in-ano are usually quite simple to manage. Most acute abscesses can be dealt with in a clinic under local anesthesia without major trouble to the patient. Those patients who develop a chronic fistula-in-ano can usually be managed by simple fist-ulotomy methods. An array of surgical techniques is available to the surgeon treating a patient with high anal-fistula, but, in conclusion, kṣārasūtra undoubtedly proves to be a superior and more successful procedure with a 98 percent success rate.
References
1. Bhaskar Rao, M. An overview of ksharasutra and its application in high anal fistula. NAMAH 2001; 8:4: 28.
2. Seow-Choen, F., Nicholls, R.J. Anal fistula. British Journal of Surgery 1992; 79: 197-205.
3. Deshpandy, P.J., Sharma, K.R. Treatment of fistula-in-ano by a new technique, review and follow-up of 200 cases. American Journal of Proctology 1976: 39.
4. Schouten, W.R., van Vroonhoven, T.J.M.V. Treatment of ano rectal abscess with or without primary fistulotomy: results of a prospective randomized trial. Dis. Colon Rectum 1991: 34-60.
5. Gracia Aguilar, J., Belmonte, C., Wong, W.D., Goldberg, S.M., Madoff, R.D. Anal fistula surgery: factors associated with recurrence and incontinence. Dis. Colon Rectum 1996; 39: 723-9.
6. Kuijepers, HC, Schulpen, T. Fistulography for fistula-in-ano: is it useful? Dis. Colon Rectum 1985; 28: 103-6.
7. Pescatori, M., Maria, G., Anastasis, G., Rinallo, L. Anal manometry improves the outcome of surgery for fistula-in-ano. Dis. Colon Rectum 1989; 32: 588-95.
8. Krongorg, O. To lay open or excise a fistula-in-ano: a randomized trial. British Journal of Surgery 1985; 72: 970.
9. Bhaskar Rao, M. Post-operative wound healing with ksharasutra — a new approach in high anal fistula. Ancient Science of Life 1995: 123-8.
10. Bhaskar Rao, M., Prasad, S.V. Multi-centre study of ksharasutra in high anal fistula. A Journal of NTR. UHS; 199: 83-7.
Dr. M. Bhaskar Rao, MD in Āyurveda, is Assistant Professor at the Department of Shalya, SV Āyurvedic College and Hospital, Tirupati.
Share with us (Comments, contributions, opinions)
When reproducing this feature, please credit NAMAH, and give the byline. Please send us cuttings.