Mental health
Memories from beyond: 'unseen' effects of trauma
Abstract
This article proposes that war and trauma have multiple side-effects. They directly damage not only soldiers, their ‘victims’ and descendants, but also the wider population indirectly as collateral. People in the general population may energetically ‘pick up’ or spontaneously access the trauma of entities who don’t know they are dead. This may cause deeply uncomfortable visionary memories, depression, or result in further acts of terror. The author provides her personal experiences when memories from beyond influenced her mind and body. She assumed that these traumatic ‘memories’ were normal, though uncomfortable and she did not pathologise them. She discusses unusual, anomalous or extreme experiences and assumes these experiences are a normal part of being human. The author explores the proposition that crisis experiences are caused both by trauma in our present incarnation and they reach us from dimensions beyond. She explores how insights may be transferable to healthcare practice.
Who am I?
In my life I have travelled a lot, held quite a few jobs, worked within many disciplines and visited quite a few countries. As a cultural anthropologist I did research in Sudan for my doctorate on material culture, housing and settlement and later travelled to India to do two projects: to study pilgrimage and sacred space; and as a medical anthropologist to explore attitudes to mental wellbeing. In 1998 I had a spontaneous visionary experience during a university conference, which I could not control. During that experience in 1998 I received insight to retrain in medical anthropology and specialise in mental health and psychiatry.
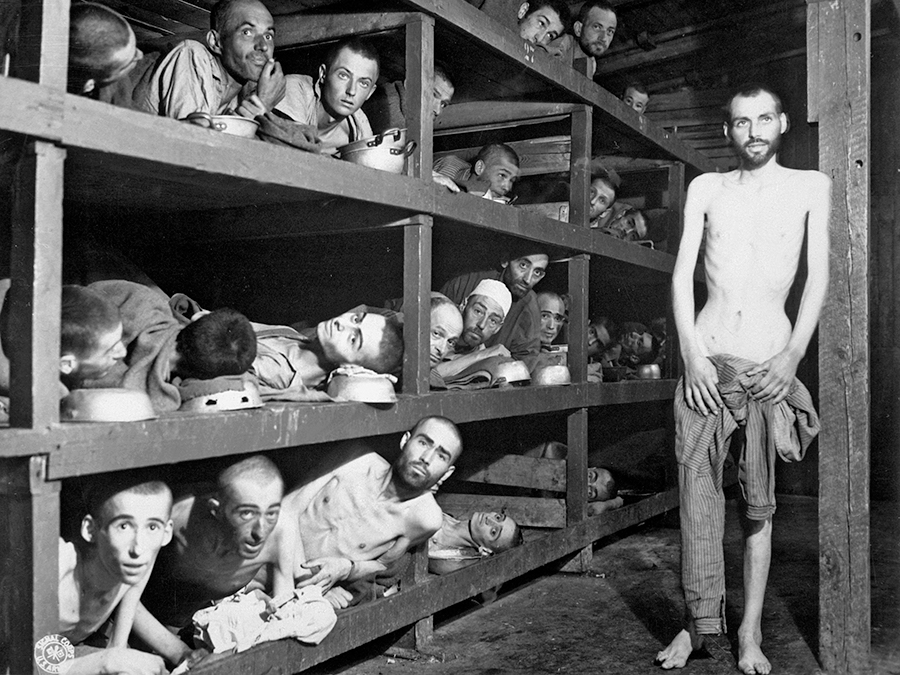
In my 20’s in this Natalie life, I spontaneously remembered life in a Nazi Holocaust experi-mental ‘hospital’, strapped to a gurney. I experienced events in technicolour detail, which I remembered for over 10 years in this life, the horrors of that life. I remember being in the gas chambers, over heating, not being able to breathe and dying. This was something I wrote for Paradigm Explorer, the journal of Scientific and Medical network:
“I was gifted these memories over ten years in my 20s and 30s: I knew who I was, as Natalie, and I could distinguish who that person there in the medical experimentation camp was. I could witness both what happened to them… and when we were led to the showers, for the final solution, I knew what was going to happen. I died angry at such a waste of shortened lives (1)”.
As far as I am aware none of my ancestors were in Nazi Germany, so how did I access that information and those experiences? In the West, some of us may use a linear model to describe our assumptions that life begins at conception or birth and continues in a linear manner until death, which is the end of the process (except for spiritists, and people originating from Non-European places on earth). Did a linear model of life fit my experiences above? No, it did not...
Multiple interpretations?
I am wondering how we might interpret my experiences: were they ancestral memories from a real (but unknown) family history, or from a past life of mine, or from someone else’s past life, or someone’s actual life, which I had somehow tuned into? Did I experience extra-ordinary empathy, or profound focused knowing or clairvoyance? Did I somehow tune in remotely to another person’s traumatic experiences, or was I able to access Akashic realms, or some other field of consciousness, in an unsolicited manner? Perhaps I had experienced spirit attachment or possession of my body and my mind? Or perhaps over those ten years of experiences I wonder if all those memories were my spiritual imagination?
Where did the data of this remote perception come from? As I said before, I always knew who this Natalie person was, but my body reacted as if it was not so aware. Did I have false memory syndrome, or not? I had always thought it could not have been epigenetics, as all my biological ancestors were already in UK before Nazi practices began, though both parents’ distant families had experienced pogroms in 19th century Russia and Poland. One psychology counsellor claimed I may have had: a memory which appeared to be new, but was recalled from TV, book or radio. His interpretation didn’t fit my own understanding.
Intergenerational trauma
These experiences made me ask myself whether I was born free. Or did I enter this Natalie existence as a new-born with a package of old experiences to address? Studies illustrate that Post Traumatic Stress Disorder can occur across generations, from people who had direct experience, to their offspring. One study found Nazi holocaust trauma in one generation passed on trauma to the next, through the genes: the theory of epigenetic inheritance. “Genetic changes stemming from the trauma suffered by Holocaust survivors are capable of being passed on to their children (2).”
An American researcher studied children of Holocaust survivors, and found descendents of those who experienced Nazi Holocaust had altered stress hormones, which predisposed them to anxiety (3). Other authors mentioned their memories of the past, beyond their birth which appeared to come from someone else’s existence, an-other’s existence. These include writings on the Holocaust and reincarnation of Yael Shahar (4), Elise Wardle (5), and Rabbi Gershom (6).
I wondered if it was possible for those who had been diagnosed with mental distress, or who have had spiritual awakening, or extreme experiences, to be responding not only to trauma from their current incarnation, but also from a previous incarnation? Or did they tune in sensitively to a current or previous life scenario? Perhaps it was possible to have PTSD from a remote memory? I discuss this material in more depth in my recent book (7).
Understanding this proposition about remote sensitivities made me question the ‘diseases of the brain’ and ‘chemical imbalance’ models of mental distress. Alongside the scientific evidence offered by Whittaker and Cosgrove (8), Whittaker (9) and Davies (10), there was a lot of material on non-local experiences and ‘memories’ that made me further doubt bio-medical models of mental ill-health.
Ubiquitous reincarnation beliefs
As an anthropologist, I conducted a couple of research projects in India, and in the most recent I interviewed priests, psychiatrists and traditional healers in temples, mosques, clinics and churches about ways they interpreted “symptoms of distress (11).” On one of my visits to Rameshwaram in South India, I saw rituals for the dead carried out on the seashore, which was a healing place for the dead, rituals conducted for mental peace, and for relatives’ closure after bereavement.
Pilgrims in India explained to me that our physical body enveloped an ethereal body. After death, cremation destroyed the first body, liberating the second ethereal body, where it would journey to the abode of ancestors. Once at the abode of ancestors, the protective case was sloughed off, the ethereal body would experience consequences of past actions, before being reborn. In India, people said a person consisted of a body, breath and a soul, and identity was not fixed at the skin.
I discovered while doing training in UK that people who were first generation migrants from India (and its diaspora) also believed an individual did not die with the human body. There were widespread beliefs that ancestors continued to exert influence over their living relatives. A human being was believed to consist of both physical and non-physical components, some of which preceded and survived death.
In addition a living person’s body appeared to be permeable to spirits of the dead. In many non-Western countries, much human misfortune and mental ill-health was attributed to ghosts of those who died an untimely death. For example belief in ghosts was ubiquitous in Asia, First Nation America, rural Africa and similarly with first generation Asian migrants. A ghost required prayers in order to become an ancestor, to be recycled and reborn as a human baby.
For many years scholars in the West assumed the only people to hold beliefs about reincarnation were Hindu communities from south Asia. However a Professor of Anthropology at Princetown University argued that India was only one place among many to hold this belief (12). Reincarnation beliefs were also central to native Americans, Africans, and Oceanic peoples.
The practitioners I met in India acknowledged Eastern and Western beliefs may be incompatible. Western models of psychiatry did not fit their spiritual beliefs about the nature of human existence. Eastern assumptions concerned rebirth and repeated incarnations, where the body was porous and could be influenced by external forces. Importantly they believed mental illness was an episode, and religion and spirituality were important to health. I too believed symptoms of distress were an episode and found certain bio-medical assumptions around ‘illness for life’ shocking.
Wondering about spiritist perspectives
I wondered to what extent my interpretation of experiences was transferable to others. Was it possible that in the West our mental health had become more severe, both as a result of unacknowledged present trauma, but also as a result of unacknowledged past-life traumatic events which resulted in sudden death? Or might people have experienced unsolicited profound empathy with an ancient person’s experience? One perspective of those who held spiritist beliefs was that when people were killed suddenly, they may not know they were dead. They may not be aware their body had died, and an aspect of their consciousness may wander around, overshadowing living people who expressed emotions they recognised (13, 14). In Tibet there is a long tradition of reciting prayers for days, to ensure no aspect of a deceased person remains clinging to earth (15).
Such perspectives and cultural understandings are not accepted universally: beliefs considered normal in some parts of the world may be considered delusional in the West. This conflict of interpretation matters because it influences how people are treated when they have disturbing inner experiences or remote perception. Particularly in the West, people who are new migrants or refugees may be pathologised. I do discuss non-Western perspectives around mental well being in much more detail in my Cultural Perspectives book (16).
It seemed that both actual and remembered trauma could equally be triggers of distress. This suggested to me that people who present to our medical and health care services with mental distress might be invited to explore narratives of their deep history in open dialogue or within counselling. However how do we start to educate staff in different ways of thinking about the self and support ways of training, asking people about their narratives? I doubt we need to know intellectually about each and every previous experience in order to release it. Perhaps we just need to hold the intention to release all traumas across all time and space? Is this spiritual or emotional bypassing as certain psychologists might suggest (17), or can we use healing strategies that are simply available to us now?
Who cares about our beliefs on mental health?
In the West there are several groups of people who express dissatisfaction with current models for mental health diagnosis and treatment. These include: culturally new migrants, refugees and asylum seekers; patients and their families with experience of the mental health system; psychiatrists who know their training does not fit the spirit of our times and psychologists aware of the importance of personal history. In addition there are original indigenous inhabitants of Australia, Africa, Canada and USA who do not want their narratives about religious experiences and altered states of consciousness pathologised by a colonial host population: they prefer their ancient practices to be acknowledged and honoured.
For decades in UK, Australia and USA, the dominant model for extreme experiences was assumed to be bio-medical, and we mistakenly assumed our diagnoses and treatments were transferable throughout the world. But we were wrong (18, 19, 20). Practitioners are more aware their bio-medical training doesn’t fit the current zeitgeist, and many are starting to question the original diagnoses of their professions. Now we need a cultural U-turn towards more insightful cultural awareness training at our medical and healthcare educational institutions.
Changes are starting to happen: The British Medical Journal reprinted an article entitled ‘Drop the language of disorder’ (21), and the Council for Evidence Based Medicine earlier published a report (22) on ‘Unrecognised Facts about Modern Psychiatric Practice’. The practice of group discussion with consent has recently taken off throughout Western countries (23), although for millennia, it was a normal practice for addressing distress by a council of elders in African countries and in USA, New Mexico elders had sacred spaces (kiva) where they performed a ceremony and held discussions. Today there is a greater understanding of a spiritual dimension, which some people access deliberately, some by chance, while others may become distressed, particularly if they have no conceptual framework for understanding the experience. In recent times there is a greater understanding of the trauma triggers of distress, plus the role of social, political, and economic inequalities.
Our personal beliefs are important: they inform the way we interpret experience: our theories of illness causation influence our health-seeking strategies for mental wellbeing, our access to healthcare and our acceptance of diagnosis and treatment.
How do we move forward?
I hope it is possible to further open the discourse around mental wellbeing: to explore consciousness beyond the brain and ways it influences people who are deemed by materialist ways of understanding, to have ‘mental health problems’ or schizophrenia. Let us meet together with all stakeholders around the same table, compare the phenomenology of experiences (with or without distress) and discuss any outmoded basic assumptions around human experiences. Let us have an open-ended enquiry around human inner experiences towards an expanded science, beyond a materialist worldview.
A recent PhD awarded to Brian Spittles (24) by Murdoch University in Australia made a significant contribution towards a better understanding of psychosis. The author provided us with systematic substantive arguments as to why radical change is required. He gathered evidence which enabled us to examine psychosis through a range of materialist and metaphysical contexts. He explored the historical ebb and flow of beliefs around psychosis; he then suggested Western psychiatry limited our scope for understanding psycho-spiritual experiences.
As well as acknowledging insights by Western scholars, Spittles also presented metaphysical perspectives from indigenous peoples and Eastern Buddhist philosophies. He invited a paradigm shift within psychiatry, similar to examples in Brazil, where mainstream doctors have worked together with traditional healers for the last 50 years. Change is occurring: in UK a new group British Spiritist Medical Association was recently set up by Brazilian scholars. Let us also acknowledge the work of Stephen Harrod Buhner (25) and support those who have what he calls ‘open gating’ with deep sensitivity to sound and environment.
Conclusion: addressing current dilemmas
I propose war and trauma not only damages soldiers, ‘victims’ and their descendants, but also the general population, who may unconsciously, energetically and spontaneously access trauma of both the living and the dead. This may cause horrific visionary memories, unattributable depression, or result in further acts of terror, that may or may not be a result of over or wrong medication. For the above insights to be sustainable, we need to ensure our education system in medical and healthcare establishments, religious experience, psychology and parapsychology departments, is up-to-date with our new understandings on culture and altered states of consciousness. The long-term aim of this work is to promote social wellbeing according to the spirit of our times. We need to work together.
There is a problem, not just with front line medical and healthcare staff, but with the education system as a whole and with politics. New students may be trained in old ways of thinking about anomalous phenomena. This is unfortunate for those who suffer from mental breakdown, extreme experiences, or spiritual emergency. We must train staff globally in plural ways of thinking.
Are we willing to collaborate?
Those of us in the academic disciplines of Religious Studies, Psychiatry, Transpersonal Psychology, Paranormal Psychology and Medical Anthropology — I am writing to ask if we could create a bridge amongst ourselves? It would be marvellous to see more profound dialogue between the various disciplines: scholars sitting together around a table, exploring the phenomenology of anomalous experiences for the benefit of those who experience mental distress. Again I invite academic scholars to compare the phenomenology of experiences which result in mental distress. Could we use our research data to compare and contrast the lived phenomena of human experience? As more people learn about other states of consciousness, this would positively enhance our global dialogue around mental health. Let us acknowledge the multiple layers of understanding for addressing health and wellbeing.
References
1. Tobert N. Thinking the Unthinkable: Ancestral Memories and Consciousness. Paradigm Explorer 3, Scientific and Medical Network 2018: 12.
2. Thomson H. Study of Holocaust survivors finds trauma passed on to children’s genes, The Guardian, 21 August 2015. [Online] https://www.theguardian.com/science/2015/aug/21/study-of-holocaust-survivors-finds-trauma-passed-on-to-childrens-genes (Accessed August 2019)
3. Yehuda R. How Trauma and Resilience cross Generations, WNYC Radio broadcasts, New York. 2015 [Online] http://www.wnyc.org/story/rachel-yehuda--how-trauma-and-resilience-cross-generations/ (Accessed August 2019)
4. Shahah Y. (Ovadya Ben Malka). A Damaged Mirror: A story of memory and redemption. Alfei Menashe, Israel: Kasva Press; 2015.
5. Wardle E. Memories of the Holocaust and Questions of Past Lives. J Psychiatry 2015. 18: 220.
6. Gershom Y. From Ashes to Healing: Mystical Encounters with the Holocaust. Virginia, USA : A.R.E. Press (Association of Research & Enlightenment); 1996.
7. Tobert N. Cultural Perceptions on Mental Wellbeing: Spiritual Interpretations of Symptoms in Medical Practice. London: Jessica Kingsley Publishers; 2017, p. 195.
8. Whitaker R, Cosgrove L. Psychiatry under the Influence, Institutional Corruption, Social Injury, and Prescriptions for Reform. New York: Palgrave Macmillan; 2015.
9. Whitaker R. Anatomy of an Epidemic. New York: Broadway Books; 2010.
10. Davies J. Cracked: Why Psychiatry is Doing More Harm Than Good. London: Icon Books; 2014.
11. Tobert N. Spiritual Psychiatries. Charlottesville, USA: CreateSpace; 2014.
12. Obeyesekere G. Medusa’s Hair: An Essay on Personal Symbols and Religious Experience. Chicago: University of Chicago Press; 1981.
13. Kardec A. (Duncan JA Transl.) The Gospel According to Spiritism Paperback. London: Two Worlds Publishing Co Ltd; 1987.
14. Palmer T. The Science of Spirit Possession. Newcastle, UK: Cambridge Scholars Publishing; 2015.
15. Baldock J. Tibetan Book of The Dead. [Online] London: Arcturus Publishing Ltd; 2013, https://www.youtube.com/watch?v=_CIVvJsQPvk (accessed August 2019).
16. Tobert N. Cultural Perceptions on Mental Wellbeing: Spiritual Interpretations of Symptoms in Medical Practice. London: Jessica Kingsley Publishers; 2017, p. 195.
17. Wellwood J. Toward a psychology of awakening : Buddhism, psychotherapy, and the path of personal and spiritual transformation. Boston: Shambala; 2000.
18. Fernando S. Mental Health Worldwide: Culture, Globalization and Development. UK: Palgrave Macmillan; 2014.
19. Watters E. Crazy Like Us: The Globalization of the American Psyche. Melbourne, Australia: Scribe Publications Pty Ltd; Melbourne 2010.
20. Mills C. Decolonizing Global Mental Health: The Psychiatrization of the Majority World. London: Routledge; 2014.
21. Kinderman P, Read J, Moncrieff J, et al. Drop the language of disorder[Online], BMJ Evidence-Based Mental Health; 2013. 16:2-3. http://ebmh.bmj.com/content/16/1/2.full (Accessed August 2019).
22. Council for Evidence-based Psychiatry. [Online] MPs and peers present case for national prescribed drug helpline to Public Health England. 2017. http://cepuk.org/2017/03/28/mps-peers-present-case-national-prescribed-drug-helpline-public-health-england/ (Accessed August 2019).
23. Seikkula J, Olson M. Therapists’ Responses for Enhancing Change Through Dialogue: Dialogical Investigations of Change. In: Borcsa M, Rober P. (eds) Research Perspectives in Couple Therapy. Cham, Switzerland: Springer; 2016.
24. Spittles B. Better Understanding Psychosis: A Psychospiritual Challenge to Medical Psychiatry. Perth, Australia: Murdoch University; 2018.
25. Buhner S H. Plant Intelligence and the Imaginal Realm. Vermont, Canada: Bear & Company Publisher. 2014.
Dr. Natalie Tobert is a medical anthropologist based in the United Kingdom.
Share with us (Comments,contributions,opinions)
When reproducing this feature, please credit NAMAH,and give the byline. Please send us cuttings.