Music therapy
Multi-sensory approaches of music in the brain — I
Abstract
The future of evidence-based treatment plans for sensorimotor dysfunctions of neurological disorders lies behind the concepts and research of ‘Multi-sensory approaches of music. In the brain’. The therapeutic use of music in the rehabilitation and development of patients with Parkinson’s, Traumatic Brain Injury, Stroke, Multiple Sclerosis and Huntington’s Disease has been well documented since the 1990s. This article provides a glimpse of three standardised rhythmic-musical applications for rehabilitation, development and maintenance of sensorimotor function.
Music therapy is an evidence-based therapy that provides the concepts and therapeutic evidence of brain processing through musical interventions in clinical settings. Whenever we are talking about musical interventions, the first question that arises is, ‘What are those musical concepts and materials which help the therapist to build conceptual musical interventions in clinics?’
This paper describes and explores the multi-sensory brain processing in music. It has three main sections. The first provides an introduction to basic musical concepts and elements in clinical improvisation. The second considers the evidence-based research on the multi-sensory approaches of musical materials in the brain. The stage for the final section describes the applications of clinical improvisation in the treatment plans for the target population.
Improvisation is a method in music therapy used by therapists in a broad spectrum of clinical populations to achieve therapeutic outcomes. It is commonly reported in extant literature as being effective within individual and group formats towards the development of cognitive, affective, sensorimotor, and communicative behaviours. Certainly, improvisation is utilised as a medium for self-expression and toward the rehabilitation of appropriate socio-emotional functioning.
This section of the article describes the basics of musical concepts and materials. Temporal, Tonal, and Timbre are three ‘T’ constructs of improvisation. The Temporal constructs include pulse, meter, rhythm, and tempo in which therapists define and organise time in music. On the other hand, the organisation of pitches, which are commonly referred to as melody, harmony, modality, and tonality, creates the Tonal characteristics used in improvisation.
Pulse is often described as a basic beat in music but some researchers have distinguished between the term ‘pulse’ and ‘beat’ by describing a beat as a single acoustic event which, when occurring at repetitive and temporally equal intervals, creates a sense of pulse that is felt rather than heard. This most basic structure of time is based on felt patterns of stable, periodically recurring amplitude modulations. One large-scale subdivision of the pulse created by the short cyclical repetition of amplitude modulation is described as ‘Metre’. A sense of metre is felt when sound is organised in groups of two (drupal) and three (triple) metre through the repetitive use of amplitude modulation within the basic beat.
Rhythms are created by fluctuating durations of each note or intervals between each note. Rhythmic patterns are the smaller subdivisions within the metrical structure of a given song or improvisation. Tempo means speed or velocity of music and is determined by the frequency rate of repetition of beats within a given time-frame. This is expressed as beats per minute (bpm) and is generally in the range of 40-200 bpm. Tempo influences a multitude of responses, from motor activity to perception of emotion, to arousal and motivation. Elevated tempi tend to require and induce increased muscle contractions, whereas slower tempi tend to be associated with muscle relaxation.
Last but not least, the other ‘T’ constructs in clinical improvisation is the use of Timbre and its effects on cognitive, affective, motor, and social responses. Variation in timbre from gentle to harsh can be utilised to facilitate different states of muscle contraction during improvisation exercises designed to aid motor development or rehabilitation (1).
The second section of this paper provides information about the evidence-based research behind the multi-sensory processing of musical constructs in the brain. Under the temporal construct, the multi-sensory perception of rhythm was studied by various researchers who drafted the findings in three-part of influences, including visuomotor, somatosensory, and movement-based influence.
Grahn and Brett described the activation of the basal ganglia, especially putamen and its connection to visual stimuli. Evidence demonstration supported the prediction that sensorimotor synchronisation to auditory stimuli tends to be superior to sensorimotor synchronisation to visual or vibrotactile stimuli (2).
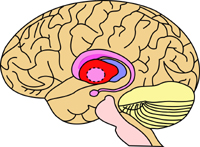
The putamen is a round structure located at the base of the forebrain. It is interconnected with many other structures in the brain and works in conjunction with them to influence many types of motor behaviours, including motor planning, learning and execution, motor preparation and movement sequences. Along with various types of movements, the putamen also affects many types of learning, including reinforcement learning and implicit learning. The auditory advantage is almost eliminated if visual rhythms are presented using continuous stimulation. Some evidence suggests that the deaf possess some advantage in tracking visual rhythms. The strength of direct visual input to auditory-motor pathways is likely enhanced in deaf individuals. Many studies have used EEG to assess neural entrainment to the beat. Dopamine is a neurotransmitter that has a dominant role in the putamen. When a cell body of a neuron in the putamen fires an action, potential dopamine is released from the presynaptic terminal and influences the substantia nigra, which affects motor planning. After discovering the function of putamen, it has become apparent to neurologic music therapists that the putamen and other parts of the basal ganglia play an important role in diseases that involve degeneration of neurons like Parkinson’s disease (PD). In PD, putamen plays an important role because its input and output are interconnected to the substantia nigra and the globus pallidus. In PD, the activity indirect pathways to interior globus pallidus decrease and activity indirect pathways to external globus pallidus increases. This is why PD patients have tremors and difficulties in performing voluntary movements and face a difficult time in motor planning.
Treatment plan
Parkinson’s disease is characterised by severe movement impairments that usually cause gait disorders which include small steps, lower cadence, reduced gait speed and sometimes festination and freezing. The research studies of Dr. M. Thaut described that rhythm and isochronous stimulation through metronome can improve the gait. Rhythmic auditory stimulation helps PD patients to improve gait velocity, cadence, and stride length and sometimes even minimise the freezing episodes. Such improvements can exist even after the absence of auditory stimulation in cueing based training programme for long-term effects and therapists can use this auditory and cueing technique intervention for gait rehabilitation. The multi-sensory processing behind this beneficial effect of Rhythmic Auditory Cueing is to enhance the neural transmitters to generate temporal expectations and help them to predict the occurrence of the next rhythmic steps. These rhythm-driven predictions and expectations can improve and regularise the motor functions of impaired temporal processing of the brain.
There are three standardised rhythmic-musical techniques based applications for rehabilitation and development of sensorimotor function:
1. Rhythmic Auditory Stimulation (RAS);
2. Patterned Sensory Enhancement (PSE); and
3. Therapeutic Instrumental Music Performance (3).
1. Rhythmic Auditory Stimulation (RAS) advocates the use of physiological effects of auditory rhythm on a motor function to improve and maintain control of movement in rehabilitation and development of patients with significant gait deficits due to neurological impairment. FMRI studies described the effects of external acoustic stimuli before and during the movements that lead to activation of dorsal premotor areas which trigger and influence the timing of movements, and focuses on oscillatory movements such as gait and arm swings. This technique is not only part of the treatment plan of PD patients but also very effective and beneficial for improving gait parameters in patients with Stroke, Traumatic Brain Injury, Cerebral Palsy, Spinal cord injuries, and Multiple Sclerosis, including gait velocity, cadence, stride length, and gait symmetry.
2. Patterned Sensory Enhancement (PSE) is a technique applied to non-biologically rhythmic movements such as arm and hand movements, functional movement sequences like dressing or sit-to-stand transfers. This musical intervention uses the rhythmic, melodic, harmonic, and dynamic-acoustical construct of music to provide temporal, spatial, and force cues for movement which are not very rhythmic by nature but which help to organise functional exercise, movement patterns, and daily life activities. For successful rehabilitation of fine and gross motor control of the upper extremities, high-intensity training with frequent repetition is very important. PSE is not only helping the patient through auditory structures to drive and enhance the movement, but also provides an additional motivational component to therapy through the incorporation of familiar songs and music, resulting in more repetitions of exercises and higher compliances with home exercise programmes.
3. Therapeutic Instrumental Music Performance (TIMP) advocates the engagement of Musical instrument playing, which requires an interaction between the sensorimotor, auditory, and visual systems. Through this technique, appropriate musical instruments are selected for therapeutic exercise to enhance functional hand movements, finger dexterity, limb coordination, endurance, and strength. In this technique, the instruments are not played in the traditional way but placed in different locations as a target to practice movements for feedback and feed-forward interactions between the premotor areas of the cortex and auditory, along with engaging the cerebellum and the basal ganglia. Repetition is extremely important for learning and training movements, TIMP exercises can give the opportunity to perform repetitive movements at various speeds and combinations, enhance fine and gross motor skills. On the other hand, through the appropriate placement of instruments to facilitate repetition, discrete movements of the fingers, arms, and legs can be trained, and eventually, sequential movements of different limbs along with bilateral engagement of both the upper and lower extremities can be trained successfully.
Conclusion
Over the last three decades, a series of evidence-based papers have set the foundation of research in ‘Music and the brain’. These papers advocate Neurological Music Therapy as an evidence-based therapy in the treatment of neurological disorders. The hidden secrets of music therapy lie behind the science of the use of rhythm and music as a tool in the rehabilitation, development and maintenance of sensorimotor functions, particularly in the treatment of neurological disorders. In this article, we have advocated the multisensory approach of music in the brain and particularly the Temporal (rhythm) structures in music remains the main element when using music in the treatment of sensorimotor dysfunction. Other musical elements can also enhance the complex motor movements such as arm and hand movements that are not very rhythmic. Three standardised techniques — Rhythmic Auditory Stimulation, Patterned Sensory Enhancement, and Therapeutic Instrumental Music Performance have become well accepted in the treatment of impairment and restoration of cortical re-organisation, motor learning, and neuro-muscular re-education. The new evidence-based treatment plan in sensorimotor rehabilitation is well accepted in the case of patients with Parkinson’s, Traumatic Brain Injury, Stroke, Multiple Sclerosis and Huntington’s disease.
References
1. Thaut MH, Hoemberg V. Handbook of Neurologic Music Therapy. Oxford University Press; 2014, pp. 24-46.
2. Grahn JA, Brett M. Rhythm and Beat Perception
in the motor areas of the brain. Journal of Cognitive Neuroscience 2007;19(5): 893-906.
3. Thaut MH, Hodges DA. Handbook of Music and The Brain. Oxford University Press; 2019, pp. 695-714.
Aradhana Deogharia is a neurological music therapist and the Founder and President of NAVYA Foundation, USA.
Share with us (Comments,contributions,opinions)
When reproducing this feature, please credit NAMAH,and give the byline. Please send us cuttings.