Surgery
The ancient principles of a pre-operative food regimen in the light of contemporary sciences
Abstract
Any bodily injury, be it operative or accidental, is not only associated with local effects, but is also accompanied by a systemic metabolic response. Nutrition, fluid and electrolyte maintenance is a fundamental component of surgery. Patients undergoing surgery are at high risk of malnutrition due to the combination of pre-operative starvation and activation of both the immune system and the neuro-endocrine stress response. Malnourished surgical patients are at increased risk of cardio-respiratory embarrassment, chest and wound infections, prolonged hospitalisation and death. Hence, feeding must be undertaken pre-operatively. Patients awaiting planned surgery should be admitted early to rectify any malnutrition and to make compensatory arrangements for potential fluid and electrolyte imbalance, which might occur during and after operative procedure. Suśruta gave strong recommendations about this in his treatise, the Suśruta saṁhitā. He advised that no surgical procedure should be performed without first administering a light, liquid diet. The principle still stands today but in other forms of administration.
Introduction
The great Frenchphysiologist, Claude Bernard, was the first to recognise that human beings live in two very different environments: the external environment, and the milieu intérieur, in which the tissues lived. After 50 years, the outcome of these protective mechanisms was termed ‘homeostasis’ by Walter Cannon, a professor of Physiology at Harvard. At the crux of this milieu intérieur is the maintenance of normal fluid and electrolyte balance (1).
Patients undergoing surgery are at a high risk of malnutrition due to the combination of pre-operative starvation and activation of both the immune system and the neuro-endocrine stress response. Starvation reduces the anabolic substrate available to the patient, whereas the immune/stress response induces whole-body catabolism. In particular, the stress response to surgery and trauma is associated with a significant increase in metabolic rate, glucose and fatty acid utilisation, gluconeogenesis, and skeletal muscle protein degradation. These factors all contribute to the depletion of protein, lipid and carbohydrate stores and deterioration in nutritional status. In turn, poor nutritional status is linked with adverse outcome via the effects of tissue wasting and impaired organ function. Loss of power and the increased fatigability of wasted skeletal muscle delays mobilisation and affect the respiratory and cardiac function, while impaired immune function confers increased susceptibility to infection. Thus, malnourished surgical patients are at increased risk of cardio-respiratory embarrassment, chest and wound infections, prolonged hospitalisation and death (2).
Suśruta’s pre-operative food regimen
At About 1500 BC, The father of ancient Indian surgery, Suśruta had advocated feeding patients prior to surgery. He mentioned that before all operations, the patient should take a light meal (3). Concentrated alcohol should be given to those who cannot bear the pain and for alcoholics. If the patient has been fed, he does not faint and being under the influence of alcohol he does not feel the operative procedure. Hence, feeding must be done pre-operatively in diseases where indicated, as mentioned. The vitality within the human being (endogenous metabolism energy), augmented by the force of vitality from outside (exogenous metabolism energy provided from outside by articles of food, etc.), is able to maintain the body made up of the five primary elements, both being complementary to each other (4).
Suśruta clearly narrated that this is beneficial for maintaining the consciousness of the patient during the surgical procedure. Food and body, both are complementary to each other, because constitutionally both are made up of five primary elements, pṛthvī, jala, ākāśā, vāyu, and agni. Suśruta had named food, which plays a role in the maintenance of vitality (Abhyantara prāṇa), as the force of vitality from outside (Bāhya prāṇa). Especially in the context of surgical procedure, it maintains vitality through:
1. nourishment;
2. maintenance of the fluid and electrolyte imbalance;
3. prevention of surgical blood-loss; and
4. prevention of the undesired effect of tīkṣṇa madya.
Anaemia and malnutrition require prolonged care and blood transfusion. Diseases give rise to cachexia. Hypoproteinaemia is often responsible for many post-operative complications such as shock, abdominal distention (due to oedema of the gastro-intestinal track), suppression of urine (due to inability to maintain fluid balance), lowered resistance to infection and impaired wound healing, etc. It is essential therefore that hypoproteinaemia should be corrected before performing the operation. The protein replacement can be achieved in two ways; orally, by giving a high protein diet and protein preparations and intravenously, by infusion of whole blood, protein hydrolysate, plasma/plasma substitutes (dextrose).When a high protein diet is not tolerable, milk can be given continuously by the drip method through a stomach or duodenal tube (5).
Any bodily injury, be it operative or accidental, is not only associated with local effects but is also accompanied by a systemic metabolic response. The main features of this metabolic response are initiated by the immune system, cardiovascular system, sympathetic nervous system, ascending reticular formation and limbic system. However, the metabolic stress-response may be further exacerbated by anesthesia, dehydration, starvation (including pre-operative fasting), sepsis, acute medical illness or even severe psychological stress and thus any attempt to limit or control these other factors is beneficial to the patient (6).
Maintenance/optimisation of the nutritional status is an integral component of standard surgical and trauma care. Nutritional supplementation for surgical patients, if administered appropriately, can be shown to enhance outcome and improve patient quality of life in a cost-effective manner (7).
Food has nutritional value and it gives sufficient strength to the patient to tolerate the discomfort during the surgical procedure. Suśruta advised administering the snigdha and uṣṇa liquid form of diet prior to a surgical procedure. Bodily fluid loss occurs during surgery and it is maintained at a routine level. If the patient is fed by some kind of supplementation pre-operatively, it will definitely help in compensating bodily fluid loss and maintenance of vitality during surgery.
All these factors endorse Suśruta’s strictures that giving nutritional supplementary liquids before surgical procedure are essential. No matter how you are giving it, what is important are the circumstances. For the drugs used in analgesia, it can be said that anesthesia has reflux action while administering and during recovery so the oral administration of food is contra-indicated pre-operatively, not even 4-6 hours before. This keeps the alimentary canal empty which is necessary to administer the anesthetic drugs.
For the maintenance of life, water is second to oxygen in importance and is more urgently necessary for life than food.About 70 % of the body weight is made up of body-fluids. To avoid potential dehydration after an operation, especially if the patient is in a febrile state, an additional fluid should be given. If the patient has lost fluid by vomiting, diarrhoea or through drainage, an extra amount of fluid and on a volume–for–volume basis should be given. A clinically dehydrated patient (10 stone by weight) will require 3600 ml of fluid, which is the fluid lost + 2500 ml of his daily requirement, i.e. about 6 litres. This amount should be given by intravenous and other routes according to circumstances (8). One practical approach to addressing abnormal fluid and electrolyte losses is to divide the types of loss into alterations in volume, concentration, composition and/or distribution.
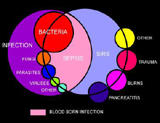
Although most patients undergoing elective surgery will derive their pre-operative fluids from normal oral intake, those undergoing emergency surgery may require fluid and electrolytes parenterally for both replacement and maintenance (9). Replacement of body fluid and electrolytes represents a fundamental component of surgical practice. An understanding of the complex mechanisms of homeostasis is necessary, as most diseases and many injuries, including operative trauma, alter the physiology of fluids and electrolytes within the body. Redistribution of body fluids from one compartment to another, as is seen in response to inflammation, infection and traumatic injury, usually results in a decrease in the volume of circulating extracellular fluid, and subsequent hypoperfusion or ‘shock’. During resuscitation of patients from shock, a strong working knowledge of normal fluid and electrolyte balance is paramount to assure rapid restoration of circulating volume and the prevention of the untoward squeals of the systemic inflammatory response syndrome (SIRS) and multi-system organ failure (MSOF) (10).
When food is available in the stomach, the peripheral blood is physiologically pooled to the digestive system by the body. This mechanism results in peripheral vaso-constriction. The feeling of cold skin after taking food is due to this phenomenon. Blood-loss will be less while giving skin incision in this condition. Furthermore the patient will have nutritional supplementation, which helps in early compensation of it and protects the patient from drowning in shock due to decreased volume of bodily fluids.
The aim of nutritional support in the surgical patient is the primary objective of post-operative care for the restoration of normal GI function to allow adequate food intake and rapid recovery. This objective should be carried out within the context of an ‘enhanced recovery after surgery’ (ERAS) protocol or a ‘fast-track’ surgery programme. Within these multi-modal codes of surgical practice, strategies are taken to minimise the surgical stress response and to avoid traditional principles of surgical care which have been shown to have no benefit, or are actually detrimental, to the rapid recovery of the patient. Patients should be managed within the context of an ERAS protocol, with an emphasis on dynamic pain-relief, early mobilisation and the restoration of normal GI function. As well as adhering to the principles of ‘stress-free’ surgery, it is important for the surgeon to have a global strategy to maintain patients’ food intake. One basic necessity is to avoid placing nasogastric decompression tubes. Nasogastric tubes are of no proven benefit and prevent restoration of normal food intake. The surgeon should provide oral fluids up to 2 hours prior to the operation and consider routine use of oral carbohydrate and fluid loading. The latter has been proven to reduce post-operative insulin resistance and thus allows the patient to respond to nutritional support more effectively (11).
Administration of concentrated alcohol creates harmful effects to the system and makes for more rapid action. The level of effect is to be maintained up to the analgesia, for if the patient passes on to the further stage, he may become unconscious, due to the alcoholic influence. Food in the stomach delays absorption of the alcohol and so the effect can also be gradually achieved. Suśruta had to maintain the consciousness of the patient with adequate analgesic effect but there was no option except concentrated alcohol for developing the analgesia; hence, he strongly advocated food before surgical procedure.
In today’s era, diet and fluid are equally important for the pre-operative preparation of the patient. A light diet is advocated on the previous day and plenty of fluid is given to the patient in order to counteract fluid loss during the immediate post-operative period. Indeed it is advisable that a jug of glucose water be kept beside the patient, who is encouraged to drink it frequently. The patient should also be administered electrolytes for better maintaining of their loss during surgery.
In ancient times there were no options in giving nutrition and fluids to the patient to counteract the loss of fluids and electrolytes which were essentially required. Therefore Suśruta strongly advocated the pre-operative food administration. Furthermore this helped to protect the patient from becoming unconscious by the effects of the procedure. Tnkṣṇa madya was administered for analgesia and to give the strength to bear the pain.
Nutritional support should be considered as a global strategy for reducing nutritional depletion and maximising patient recovery. The correct use of nutritional support can inhibit the deleterious effects of the metabolic stress-response on patient nutrition; it can accelerate recovery in elective surgical patients and can be life-saving in malnourished patients, especially those who develop major post-operative complications. Further studies are required to optimise both the composition of current foods and their application.
Conclusion
Suśruta strongly advocated pre-operative food intake as it was important to maintain the patient’s consciousness during a surgical procedure. Food as nourishment plays an important role in compensating the loss of bodily fluids and electrolyte imbalance during surgery. Today too, it should be taken under consideration and ideally patients should be given a nutritional diet prior to surgery. It is a fundamental component of surgery to maintain the replacement of bodily fluids and electrolytes to prevent shock.Suśruta advised giving bland and warm food, consisting mostly of liquids and less of cereals, just before surgery (12). In addition to specific preparations, as per the requirement of the disease and type of surgery, food having the characteristics of yūṣa and yavāgūrpeya, can be administered. The food in the stomach inhibits immediate absorption of alcohol and gives sufficient time for the controlled effect of alcohol and prevents undesired effects. In those times, the only option to administered nutrients during surgery was oral administration. This results in less haemorrhage as the food in the stomach prevents the patient going into an unconscious state under influence of alcohol. In addition the food can provide early replacement of the fluids and loss of electrolytes.
In the present era, this concept is deferred because of availability of better anesthetic agents. The drugs are not given orally but by other parental roots of administration but the principle of fluid maintenance stands with the administration of IV fluids as a compensation of fluids and electrolytes are administered during the surgical procedures. Suśruta advised a liquid diet orally prior to surgery whereas in today’s multi-dimensional technical era it has become possible to administer the nutrients during surgery along with the administration of efficient anesthetic drugs. Administrating nutrients through routes other than oral is more useful for preventing post-anesthetic complications like vomiting.
Advantages of taking food prior to surgery |
Disadvantages of taking food prior to surgery |
| • Increases the vital strength of the patient (13) • Prevents complications like unconsciousness or shock (13) • Reduces blood loss (13) • Reduces pain due to sharp instrument application (14) |
• May develop complications like vomiting and swash (dyspnoea) (15)
|
References
1. Bland KI, Csendes A, Sarr MG. General Surgery: Principles and International Practice. 2nd ed. London: Springer-Verlag London Ltd; 2009, pp. 13-4.
2. Ibid., pp. 23-4.
3. Singhal GD. Ancient Indian Surgery, Vol. 1 (based on chapters 1-27 of Sūtrasthāna of Suśruta saṁhitā). 1st ed. Varanasi: Chaukhamba Sanskrita Pratishtan; 1981, p. 91.
4. Ibid., p. 309.
5. Das K. Handbook of Operative surgery. 5th ed. Kolkata: Author publisher; 1966, p. 16.
6. Bland KI, Csendes A, Sarr MG. General Surgery: Principles and International Practice. 2nd ed. London: Springer-Verlag London Ltd; 2009, pp. 23-4.
7. Ibid.
8. Das K. Handbook of Operative surgery. p.16.
9. Dietary Reference Values for Food Energy and Nutrients for the United Kingdom. COMA Report on Health and Social Subjects No. 41. London: HMSO, 1991.
10. Bland KI, Csendes A, Sarr MG. General Surgery: Principles and International Practice. 2nd ed. London: Springer-Verlag London Ltd; 2009, p. 14.
11. Bland KI, Csendes A, Sarr MG. General Surgery: Principles and International Practice. 2nd ed. London: Springer-Verlag London Ltd; 2009, pp. 23-4.
12. Singhal GD. Ancient Indian Surgery, Vol. 1. (based on chapters 1-27 of Sūtrasthāna of Suśruta saṁhitā). 1st ed. Varanasi: Chaukhamba Sanskrita Pratishtan; 1981, p. 145.
13. Ghanekara BG. Suśruta saṁhitā with Āyurveda Rahasyadīpika commentary, Sūtrasthāna. 1st ed. New Delhi: Meharchanda Lchmandas; 1977, p. 110.
14. Gananathasen S. Suśruta saṁhitā with Bhanūmatī commentary, Sūtrasthāna. 1st ed. Varanasi: Krishnadas Academy; 2001, p. 46.
15. Vaidya Jadavaji Trikamji. Suśruta saṁhitā with Nibandhasaṅgraha commentary, Cikitsāsthāna. 1st ed. Varanasi: Krishnadas Academy; 1998, p. 431.
Sanskrit definitions
Abhyantara prāṇa — in-breath/inner breath
Agni — fire
Ākāśa — ether
Bāhya prāṇa — out-breath/outer breath
Jala — water
Pṛthvī — earth-principle
Snigdha — oily, sticky
Tīkṣṇa madya — an intoxicating drink made from anything pungent or acidic
Uṣna — hot/pungent, acrid, sharp
Vāyu — wind
Yavāgūpeya — drink made from rice-gruel
Yūṣa — soup, pea soup
Dr. Dipsinh Chavda is Professor and HOD at Shalya Tantra Department, G.J. Patel Institute of Ayurvedic Studies & Research, Anand, Gujarat
Share with us (Comments,contributions,opinions)
When reproducing this feature, please credit NAMAH,and give the byline. Please send us cuttings.