Aim of medicine
An armchair view of physicians and patients
Abstract
Physicians are exposed to varying degrees of professional, scientific, administrative, commercial, personal and behavioural challenges. Despite these, they try to do their best to deliver, upholding the best standards of their profession. One of their main challenges is to handle a baffling variety of patients they come across. In our stressed-out times, The Hippocratic Oath might appear to be relegated to the background, but it is surely alive and kicking. While physicians deserve to be applauded for their inner resilience, most patients need to resort to spirituality to improve upon theirs.
Those who practise as physicians in our society are increasingly being looked upon with some suspicion. Dig a little deeper and one is apt to find that they are more to be pitied than censured.
A physician is denied the fundamental right to some solitude. Even at a social gathering, he is likely to be surrounded by wannabe patients who are keen to seek his impromptu advice as to the latest affliction the party has heard about and imagines he or she to be suffering from.
Close relatives are not too considerate either. A distant relative might call late at night, skilfully steering the conversation from children’s career prospects to the current bout of migraine he happens to be suffering from. If anyone in the circle of friends or relatives happens to be admitted to a hospital, the physician ends up spending sleepless nights, adroitly juggling his official commitments and personal relations, often messing up both.
Latest advancements in medicine keep them on their toes. So does the competition from various streams of medicine, such as Homoeopathy, Āyurveda, Yūnānī, Siddha and many other local variants of each of these streams. Superstitions, local beliefs, religion and social norms are but some of the constraints which need to be kept in mind. Legal tangles, such as those that apply to road accident cases, keep them on the defensive.
In advanced countries, they face tough customer care regulations. In emerging economies like India, they suffer humiliation — occasionally violent — at the hands of irate relatives and well-wishers of patients if the latter perceive the medical service provided to their kith and kin to be deficient.
Return on Investment considerations
To be a mere graduate in any discipline of medicine does not amount to much these days. Even to become a graduate, the hapless souls have to experience at least five and a half years of the tyranny of the classroom, with the trauma of a stint as an intern thrown in for good measure.
Monetary rewards obviously vary depending upon their choice of a career. They could choose to be in their own private practice, or join a private sector outfit or become a part of the public health delivery mechanism.
If public spending on the health infrastructure is woefully inadequate, private players end up playing an important role in the medical education scenario. Many aspiring physicians opt for a private sector skill provider. As a consequence, hassled parents end up shelling out sackfuls of the green stuff. Return on Investment considerations then determine the choice of their career.
The blue-eyed ones
The resourceful ones set up their own practice. If the going is good, some of them end up laughing all the way to the bank, what with hefty commissions coming in from such allied medical service providers as marketers of branded medicines and diagnostic clinics.
Those who happen to be associated with five-star private sector health facilities have tough business targets to meet. This is not to say that patient care necessarily gets compromised, but an overdose of medical investigations surely leaves the patient and her family deprived of mental peace and some hard-earned green stuff.
When the costliest of medicines and gadgets get recommended by physicians, stakeholders of pharmaceutical companies and those in the field of medical equipment laugh all the way to the bank. Admittedly, quite a lot of money gets pumped into research and development, but it is open to debate as to how much profit could be considered rational and socially justified.
Much like the marketing honchos in the private sector who bring in business and resultant moolah, such physicians happen to be the blue-eyed boys of any entity which boasts of being a corporate facility.
The grey-eyed ones
Physicians who are part of the government healthcare-delivery system and happen to be conscientious by nature are often overloaded with work. Monetary rewards are often not commensurate with the efforts being put in. The eyes of a majority of them would be a dull grey, revealing a soul which is tormented and has given up hope.
Besides having to publish research papers in peer-reviewed journals and making presentations at medical seminars, students have to be guided, examinations have to be conducted and internal meetings need to be attended. Administrative chores cannot be ignored.
Above all, routine patient care cannot be made to suffer. Patients, whether of the ‘in’ or the ‘out’ kind, descend in droves, all eager to jump the queue and catch the attention of the physician. The plight of people in most of the emerging economies is most distressing because the per capita availability of physicians leaves much to be desired.
The Patient Satisfaction Quotient
It is well-known that the Patient Satisfaction Quotient is a function of various factors — the time spent with the physician, the quality of interaction, the seniority of the physician in the system hierarchy, etc.
It follows that the following laws might apply:
Law #1: the more the time spent with a physician, the higher the level of satisfaction of a patient.
Admittedly, this law does not apply to those perched on a dentist chair. Nor does it apply to those facing a minor surgical procedure without the aid of analgesics.
Law #2: the better the quality of interaction, the higher the level of satisfaction of a patient.
This law is a direct derivative of the psychology of the individual. The more a patient is able to off-load his worries and anxieties onto the hapless physician, the happier he is apt to feel.
There are some exceptions here as well. A physician found making an inappropriate remark about the weight of a patient who is a member of the female of our species will risk losing the latter’s goodwill.
Law #3: the patient satisfaction level is directly proportional to the seniority of the physician being consulted.
Amongst the well-heeled patients, the respect and admiration for a physician depends upon the amount of fee being charged, the waiting period to get an appointment, the seniority of the physician in the system and the value as well as the rare availability of the medications being prescribed.
This one surely does not apply to the teeming multitudes who strive to keep their body and soul together day after day.
It follows that most patients using the public hospitals are left dissatisfied. It does not occur to them that the sheer exposure of such physicians is so very wide that the medical advice they dish out is much better. Superfluous investigations are discouraged. Medications recommended are often of a generic kind, saving the patient some precious money.
A Patient Motivation-Hygiene Proposition
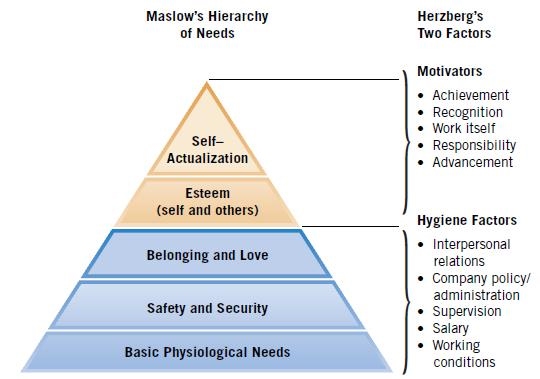
Those familiar with Herzberg’s two-factor theory, popular in the realm of organisational behaviour, would notice a striking similarity between the situation envisaged in organisations and the one we are endeavouring to explore here.
In case of organisations, job satisfaction and job dissatisfaction are not part of a continuum. Absence of satisfaction does not necessarily imply presence of dissatisfaction. If the presence of Motivation Factors (respect and recognition on the job, for instance) improves job satisfaction levels, the absence of Hygiene Factors (such as physical working conditions, etc.) leads to higher job dissatisfaction levels.
Likewise, satisfaction/dissatisfaction levels of patients perhaps tend to be independent of each other. If the treatment is effective in the long run, the satisfaction level improves. If the time spent by the physician is inadequate, dissatisfaction sets in.
In that sense, Effectiveness of Treatment would be akin to a Motivation Factor in the theory propounded by Herzberg. However, the set of laws proposed above would be like Hygiene Factors, the absence of which would cause a patient dissatisfaction.
Patients of various hues
Patients obviously come in various body sizes, pocket sizes, shapes and hues. Amongst those who do not face a medical emergency, there are wide variations in temperaments. Here are some which might be of interest.
The reluctant ones
These are patients who believe that a doctor should be visited only as a last resort and that medicines need to be stopped as soon as the immediate problem is addressed. They believe that there is no need for any follow-up visit, till, of course, the next crisis strikes.
The casual ones
These are the ones who are casual in their approach. They may or may not follow either the doctor’s prescriptions or the food restrictions placed on them. Nevertheless, a medical consultation is akin to a pleasurable outing for them, so they shall keep coming back to see the physician. For a public service doctor, they happen to be a nuisance. For those in the private sector, they are a source of delight.
The conscientious ones
In this category fall the hapless and anxious souls who take their illnesses rather seriously. They take medicines regularly, and follow diet-related advice to the best of their ability. They tend to seek guidance at frequent intervals. Those who suffer from lifestyle diseases often end up forging a close bond with the physician, thereby replicating the age-old system of ‘family doctors’.
The anxious ones
Then there are the well-heeled hyper-anxious ones who take a magnified view of their afflictions, tend to be jumpy, worry excessively about prognosis, and keep troubling the physician concerned with inane queries from time to time.
Of attitude and inner resilience
Much depends on the attitude of a patient. One could come across persons with a cheerful disposition headed for their second open heart surgery, relishing a deep-fried item with much glee. One could also run into those who worry endlessly over such transient ailments as a bout of common cold or sinusitis.
Physicians obviously deal with a baffling variety of patients with much finesse and aplomb. Nerves of chilled steel get deployed. A sense of detachment pervades their handling of a patient. Their inner resilience deserves to be applauded.
With such fine qualities of head and heart, one can merely admire the quality of their work which keeps upholding the reputation of their profession. The Hippocratic Oath might appear to be relegated to the background, but is surely alive and kicking.
In many streams of alternative medicine, the patient is taken as a composite whole and treated holistically. The inner resilience of a patient is accorded a higher weightage. Allopathy, the mainstay of masses in the times we live in, does it the other way round, where each organ is looked at and treated separately. In mathematical parlance, alternative streams could be likened to Integral Calculus, whereas allopathy could be likened to Differential Calculus.
Shoring up one’s inner resilience
There are indeed ways for patients to improve their inner resilience, so as to be able to handle the harsh slings and arrows of Fate in a more positive manner. A deeper inner connection helps. To achieve the same, regular introspection and meditation helps.
It stands to reason that almost all spiritual masters exhort one to simply disallow negative thoughts to gain a foothold in one’s psychical system. Patients obviously need loads of patience to be able to put this advice into practice!
Inputs from Dr. Shivani Salil and Dr. Shruti Bhatia are gratefully acknowledged.
Ashok Kumar Bhatia is a management advisor and writer who lives in Pondicherry, India. He blogs at www.ashokbhatia.wordpress.com.
Share with us (Comments,contributions,opinions)
When reproducing this feature, please credit NAMAH,and give the byline. Please send us cuttings.